Yves here. Note that the original chart at Bruenig’s site is interactive, so you can view the values at each data point (as in number of estimated deaths)
By Matt Bruenig, who writes about politics, the economy, and political theory, with a focus on issues that affect poor and working people. He has written for The Washington Post, Los Angeles Times, The Atlantic, The New Republic, The American Prospect, In These Times, Jacobin, Dissent, Salon, The Week, Gawker and at his home base of sorts: Demos’ Policy Shop. Follow him on Twitter: @mattbruenig. Originally published at his website
Five separate people were bylined on a Center for American Progress post about how many people AHCA will kill. The post is quite long, but all the authors really do is take the CBO estimates of how many people will lose coverage under AHCA and then divide that number by 830. They do this because there is a study that shows that 1 person dies unnecessarily for every 830 people who lack health insurance.
I have duplicated CAP’s efforts here, but rather than focus only on the AHCA, I have also included Obamacare and single payer into the mix. One other difference is that I track cumulative deaths between 2017 to 2026 rather than reporting an annual figure for each year.
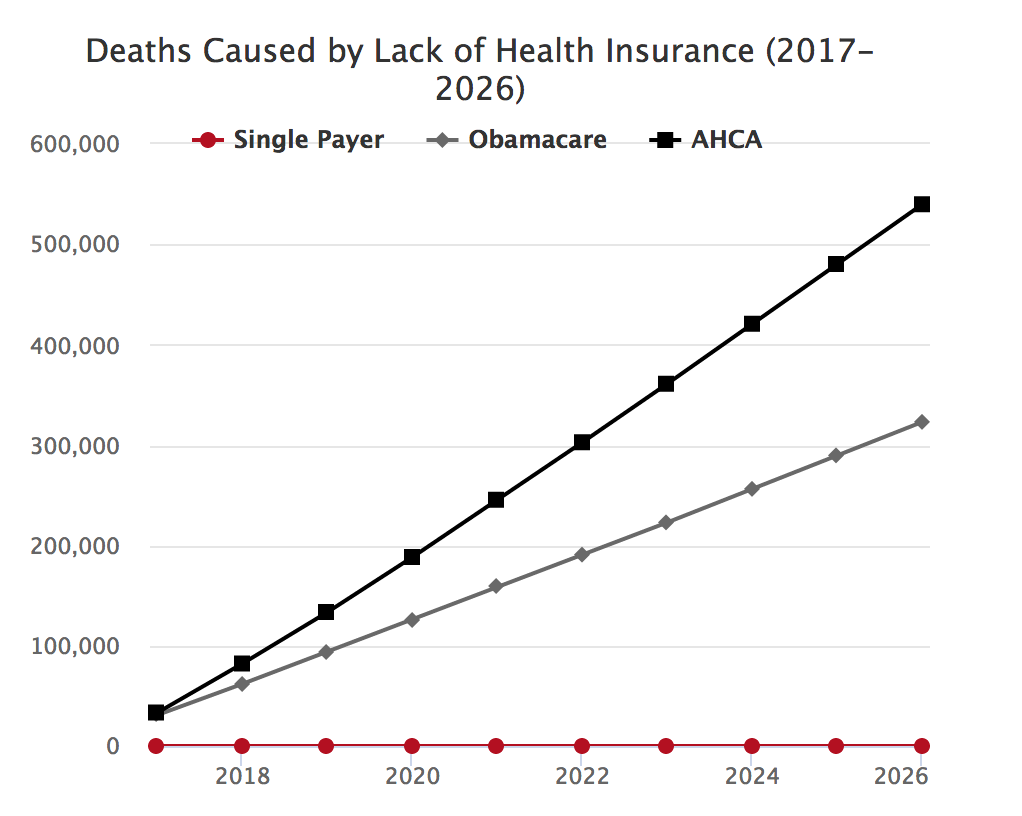
Under AHCA, nearly 540,000 people will die in the next decade because of lack of health insurance coverage. For Obamacare, it is a more respectable 320,000 deaths.


Can single payer be promoted as an economic stimulus? Money pumped into the economy as investment in health. I figure that money would go out into the economy everywhere there are people going to the doctor. Much better than top down stimulus in my estimation. MIght even encourage a resurgence in General Practitioners if it’s handled right.
Add five percent (WAG) to payroll taxes and no upper wage cutoff. Social Security Administration hires a significant amount of former insurance company employes, injecting more wages all over the country if the bureaucracy can be spread out to at least one SSA office/processing center per state.
I’m looking at Federal Wages as a net good as long as they are spread out nationally, rather than concentrated, I’m looking at DC Metro specifically. Get individual states on board as you will be creating jobs in each state. Health Barrel spending, if you will.
There are “studies” which assert that single-payer will bankrupt the government. Of course, those are as BS as gun control doesn’t work. Europe has demonstrated that single-payer does work.
The argument against single-payer is smoke and mirrors. It is really about the survival of a line of business in the insurance industry – the one that makes political donations to legislators. Oddly, Europe again shows that private insurance still exists, and like in the US, is most common among the wealthier citizens. Thus, the freedom-of-choice argument is hollow nonsense.
I have observed that part of the problem with single-payer studies is sloppy attention to the complexity of the current profit-oriented web of healthcare compensation. For example, studies often do a sloppy job of addressing the effect of removal of for-profit insurance companies from the equation. Even sloppier is how analysts attend to the complex costs (including overhead) of running complementary state programs. It is hard to fully back those costs out of the equation. The assumptions that need to be made in such studies allow the same economist to demonstrate either disaster or nirvana with the same data.
A wild card that should lower costs is timely healthcare. There is a mountain of research showing that when poor people (or rich ones) see the doctor when it starts to hurt, it is far less costly than waiting until the organ fails or the tumor bursts. Thus, some agent-based modeling would need to be done to show projected savings say over 10 years.
Lastly, healthcare politicians should answer the Sarah Palin question; “How’s that workin’ out for ya?” Over 70 years of experience with private health insurance leads to but one conclusion – it ain’t workin’ out at all.
How is single payor going to fix the rising cost of the healthcare industry and the way healthcare is delivered? Single payor is just a means of paying for healthcare without controlling cost.
1. Single payer reduces a medical provider’s overhead as there is only one account, one set of procedures, etc. that providers have to deal with. Lower overhead means less pass-through cost. Worst case, providers keep the money and billing stays the same. Best case, providers lower prices. in either case, the number of middlemen drops to one which vastly reduces the amount skimmed by insurers/banksters.
2. Single payer maximizes bargaining power, resulting in lower costs for services and treatments
3. Single payer puts all of the people into one risk pool (people paying in to cover the cost of care for those people) which results in the lowest premiums possible IF premiums are necessary at all (MMT).
4. Single payer eliminates the need for employers to provide insurance to employees and their families. Businesses will surely keep that and pay it out as executive bonuses, but the employee share (premium, deductible, copays, etc.) is pocketed by employees, providing an economic stimulus.
5. Since medical coverage would no longer be tied to an employer and their risk pool, there would be a lot of retirements and startups, which may provide an economic stimulus.
Those are 5 ways I thought of, off the top of my head, that would reduce cost of care either directly or indirectly.
There are more.
Shorter: a “single payer” can and would dictate prices and practices, besides lowering administrative costs – dramatically, considering the record of Medicare.
As it stands, doctors are reluctant to take Medicare patients precisely because it dictates payment; but it isn’t the only payer.
My understanding is another reason they don’t like Medicare is it is VERY slow to pay. That could and should be remedied.
Yves:
Medicare pays like commercial healthcare insurance. University of Michigan takes Medicare people in as well as Medicaid. My own PCP has said he has seen people on Medicaid who have never had a doctor’s appointment in the past.
There is no where I have seen where single payor is called out in the way as detailed. Conyers bill does not do it and neither did Sanders.
Single payer works lmao, Take a good look at Sweden, its almost bankrupt and Canada and France are not far behind. If it wont work in a socialist economy its never going to work in a capitalist economy! Then who are you going to assign to make the tough decisions as to who gets bed or when all treatment is cut off! Case in point UK couple told there was no hope to save their baby by UK health care but raise the money to bring daughter to US. UK steps in and says no your baby will die here! As I said who gets to play god in your idea? As to the rising cost of health care all that can really be done is to have a government/healthcare commission to assign costs to every procedure unilaterally through the country including the dispensing of pharmaceuticals. Meaning ie.. that for instance an angioplasty costs the same no matter what hospital you get it done at in the country, and the same with everything else. The only thing really that couldn’t be charged this way would be emergency medicine for things like stabbings or gunshot wounds, most vilolent traumas! But the drugs used could be!
Well, yes, if one assumes the powers that be actually want to create jobs instead of endless grift for the c suite.
One might also argue that single payer would save businesses money on health insurance for their employees, and that would be particularly good for small businesses. Of course that would assume that tptb have a use for small businesses other than as a totemic beneficiary of tax reform.
Stuckler and Basu argue that health spending results in economic growth in the Body Economic (2013). There are a number of factors related to health and economic activity. For example, less absenteeism, less drag on productivity (having to train new people as trained workers go off long term sick or die), as well as the effect of spending providing income for consumption.
This is persuasive because, as we all know, only dollars count. Well, we are lazy, so we only count dollars, ‘coz they’re easy. Pain, suffering, and/or happiness of actual people, let alone other creatures, mountain tops, the air, the climate — that’s too hard! Can’t put a tidy $ value on it, so just ignore it. Besides, it might give us numbers we don’t like.
Funny thing, I seem to remember a book written back in the 70’s, “Small is Beautiful, Economics as if People Mattered”. Wouldn’t *that* be nice!
See Gerald Friedman’s funding proposals PDF for HR 676, page 6 Figure 2: Change in after-tax household income due to adoption of progressive financing for HR 676: 95% of Americans are better off under a single-payer system.
Add that to the hundreds of billions collectively saved by eliminating administrative waste associated with the for-profit insurance industry and more potential savings from reducing pharmaceutical prices. If that’s not economic stimulus I don’t know what is.
The multiplier should actually be much better than that.
The real stimulus would come not from more money being spent on healthcare. Since all countries with socialised health systems spend a lower % of GDP on healthcare than the US does on its privatised system, single-payer should mean lower total healthcare expenditures. The actual stimulus effect would come from the mass of the population having much or their disposable income freed up that they were previously forced to allocate to unproductive insurance companies– a de facto upwards income redistribution.
Single payer, on the other hand, would be one type of Steve Keen’s “QE for the masses” that would benefit the economy as a whole because lower income brackets are more likely to spend increased disposable income on job-creating consumption that boosts aggregate demand and the economy in general.
And add to that multiplier effect yet another: the well-being that comes from knowing you live in a society that actually cares whether you live or die, and how healthy you are in the meantime.
I was on Washington state’s Medicaid expansion. It was awesome. And I chose that word carefully.
I’m 50something. New and sometimes excruciating ailments come up more and more, any one of which would bankrupt me. When I was uninsured, every little normal ache or pain came with the terror that I’d either have to live with a debilitating condition I couldn’t afford to treat, or be saddled with crushing debt the rest of my miserable life.
Multiplying that terror was pure outrage. It’s outrageous that, in this bestest of all possible countries evah, I couldn’t go to my doctor with a problem unless someone makes not just some money, but enough to satisfy insatiable greed.
When I was on AppleHealth, though, it was truly awesome. I was in awe of the fact that my society cared enough about me to see to it that I could take care of the entirely predictable effects of living long enough. The whole world was a bit more park-like. Going to the doctor sans the exchange of money was beautiful. That kind of benefit is surely hard to calculate, but, IMNSHO, it’s the whole damn point of society.
But now that I’m working 7 days, 3 nights, and every other weekend, I’m ripe for the plucking (yes, I mixed those on purpose). I get plucked for 2/3 of my food budget every month to pay for a policy I can’t afford to use. I’m back in that same terrible condition as when I had no insurance.
I was about to spend that money on a car payment, or invest in some property to develop with a friend who’s also living with family.
The feeling I get now is decidedly un-park-like. It’s just a jungle with indoor plumbing. There are monsters out here who, spider-like, would trap me in their webs and slowly suck the life out me, all while being lauded as the very model of the modern neoliberal.
So in addition to the dollars and cents, there’d be a perhaps incalculable and yet very real well-being multiplier effect.
Rabid:
How many countries have socialized healthcare?
1. Deaths are primarily caused by aging and other natural causes
2. Deaths are secondarily caused by lack of health care insurance, wars, accidents, self abuse, suicides
3. Inevitable mortality is primarily reducible thru good self care
4. Mortality is secondarily reducible thru good medical care
If you want to reduce mortality, encourage good self care … and provide good medical care. Health care insurance is a stupid way to provide good health care … like pushing a rope, for a profit. A better way would be providing universal free vouchers … and having the State compensate the medical community for each voucher accepted. And then auditing the voucher system against medical professional abuse.
That people die, suffer, or go bankrupt for reasons other than lack of universal access to comprehensive healthcare is a strawman argument against providing universal access to comprehensive healthcare.
No country that provides universal access to comprehensive healthcare has done so using vouchers. They have lower costs, better outcomes, and many incentives and practices that promote preventive care and healthy choices.
It is correct that for-profit insurance isn’t an effective way to provide access to healthcare. That’s why countries that provide universal access to comprehensive healthcare have eliminated it, as does HR 676.
tl;dr — It’s all your own fault for dying early.
You don’t need to be so vague.
1) Beyond a certain age, deaths are primarily caused by aging and other natural causes
2) Up to that age, deaths are primarily caused by lack of health care (n.b. insurance is an implementation detail), wars, accidents, self abuse, suicides
After that, the question of what the “inevitable” mortality is “reduced by” primarily depends on what you’ve got that’s killing you.
Loblolly wrote: Can single payer be promoted as an economic stimulus?
Pretty to think so, but come on — most years the U.S. medical-industrial complex spends more money buying Washington pols than does Wall Street.
Lobbying / Top Industries
https://www.opensecrets.org/lobby/top.php?indexType=i
That’s the determinant ensuring the U.S. healthcare status quo currently remains as it does. Because from any other angle — for instance, the reality that providing health insurance for their employees makes American companies cripplingly uncompetitive globally in many cases — the system makes absolutely no sense.
So, while single payer spending could theoretically be promoted as economic stimulus —
[1] However much money the Federal government puts on the table, the medical-industrial complex will pay the pols so that as much as possible ends up with Big Pharma and the health-insurance corporations. And we know that because that’s already the case: the U.S. already pays twice as much per capita in healthcare costs than almost anywhere else in the developed world and yet has the worst outcomes, etcetera, etcetera.
[2] We also know that because we’ve already had the Federal government kick in large sums of money via Obamacare/Romneycare. When I did healthcare journalism during the first decade of this century, I saw scenario studies paid for by the drug companies predicting the system’s collapse around 2020, because costs would have risen so much by then that enough Americans would be forced out of it. The result of this was the ACA, which was designed as a preemptive bailout — the medical-industrial complex getting its payoff just like Wall Street had.
[3] Beyond that there are the ancillary problems, which ramify as far as the eye can see. Single payer would obviate the need for health insurance corporations, which beside the payoffs they provide Washington pols, employ approximately 2.5 million Americans.
https://www.statista.com/statistics/194233/aggregate-number-of-insurance-employees-in-the-us/
Single payer would also over the long run tend to control doctors’ incomes. Doctors leave school with between a quarter of a million and half a million in student debts on average, last I looked. How would they pay off that debt? To what extent would American universities collapse if doctors couldn’t pay that debt?
—
[4] Nevertheless, of course, the system is unsustainable. How will it collapse?
In fact, we’re right on course for its predicted collapse circa 2020. I suggest that one way it’ll collapse is exactly what we’re seeing: the rich have bought the politicans — in this case, the Republicans — so that they don’t have to pay the taxes to support the Federal government’s preemptive bailout of the medical-industrial complex.
Hundreds of thousands will die unnecessarily and in response there’ll be more events like the shooting of Steven Scalise.
That’s how it’ll end. It’ll be that ugly and that simple.
tl;dr – you can never have nice things.
I followed this link and I read it as giving the employment figure 2.5 million for the whole insurance industry. Is that right? If so you’ve over-estimated the employment problem by a good deal.
An earlier study, done I believe in 2008 estimated that the impact of single payer would be to create a net of 2.6 million new jobs in the US in all sectors. Job losses entering into this calculation were estimated IIRC at about 400,000, which is what made me think that your 2.5 million number may be an oversight.
Thanks for pointing that 2008 study out to me and if it’s right that at least is encouraging.
Health care is currently framed ad nauseum in economic terms – single payer, bending the cost curve, coverage, etc.
Perhaps unnecessary death and suffering is a humanitarian crisis, and addressing this fact head-on is how it should be “promoted.”
Health-care is a captive market. Private industry will never compete to lower prices for patients whose only alternative is to get sicker and sicker until they die many years before they otherwise would have. Strong government intervention is the only way to meet the health-care needs of the captive patients. That continued failure to keep captive patients alive as long as they’re willing to live would result in fewer aggregate business transactions is far the weaker reason for universal health care.
Single payer does not address COSTS – Unless we all of the sudden get a CONgress that will stop selling us out to their wealthy donor bases, neither Republicans or Democrats have an incentive to change a single thing. Well, at least until some are found hanging from lampposts.
This was a response from a CEO of a major health care operator in my state (MA). It was in response as to why I have not been to my PCP for years and if I would still like to use my doctor. For those of us in the true middle class, doing ok today, but not well enough to not worry, routine and preventative healthcare expenditures no longer fit in our budget. I told them we can no longer afford to be nickel-dimed to death as spouse is on lifetime medication/care, and we fall just under our $12K deductible threshold every year to be “covered” – so nearly $12K of our income goes directly to healthcare out-of-pocket before any of us can even use “insurance”:
So to hell with Democrats that gave my family this pile of shit, and to hell with Republicans that will probably make our situation worse. Let it all burn.
from what you odescribed i am guessing you have one of those high deductible ‘insurance’ plans. i tried those too, decided to go back the ‘normal’ plans the premiums were low [mainly cause it didnt cover much) but we also had that health ‘savings’ thing to go with it. course the cost for both are more that the cost of the normal plan, only they covered a lot less. and i suspect those limited plans are what insurance wants us to have, more than either does. course they pay the politicians to push them
ahhhhh, a winner! “Single payer does not address COSTS.” Thank you for saying this. Let me add to this; Not only does Single Payor by itself (unless specified) does not control the healthcare industry costs (which most people do not understand); it also does not control the cost of how healthcare is delivered (fee for services). Atul Gawande, Uwe Reinhardt, Maggie Mahar, Donald Berwick (Head of Medicare 2008), Ezra Klein, etc. all thank you. You get it . . . https://www.washingtonpost.com/news/wonk/wp/2014/01/13/what-liberals-get-wrong-about-single-payer/
Now a bugaboo; ~$12,000 in Out-of-Pocket may not be the same as deductible. That is the maximum out of pocket including deductible. You can get a lower deductible and you v=can also get the negotiated rate for healthcare services too. You have to ask for it the same as asking for out-of-network cost negotiation if out of network emergency hospitalization.
I do not know what your situation is financially; but, you can get a lower deductible under the ACA.
Surely the cost of unnecessary death exceeds the cost of universal healthcare. Every monthly Social-Security benefit check that the unnecessarily dead never cash nor spend on neither food nor medicine, nor even property taxes, entails fewer business transactions, fewer wages earned and fewer Federal receipts.
It used to be that the business of business was business–not rent-seeking expropriation.
Clearly Single Payer is the undisputed winner, but there is a data set that should be included on this graph, which is the cumulative deaths from lack of health insurance that there would have been under whatever you want to call that mess that predated Obamacare. Both for completeness, and to see how the AHCA compares to Mad Max healthcare.
Why do these studies equate health care with health insurance???
Because they’re studies produced in the U.S.
They don’t equate health care with health insurance. Rather, they assume that some people without health insurance will not get health care that they would get if they had health insurance.
which is true, cause care is expensive, and all of our budgets are tight. and you cant budget for it.
No amount of calling what is significantly for-profit 3rd-party-intermediated (dubious value-add) pre-payment “insurance” will make it so. U.S. annual per capita health care cost is now pegged at roughly $10k. Given the annual commercial market policy churn (and notwithstanding that adult UTIL risk is roughly a 60 yr proposition “hockey stick” correlated with age), it should be unsurprising that health “insurance” companies are trying to extract that $10k from everyone every year, one way or another (e.g., high deductibles and “coinsurance”). e.g., In 2015 I was diagnosed with and treated for prostate cancer. My total OoP for the year came to right at ten grand (BCBS customer at the time, now a Medicare bene).
Another thought: ALL stakeholders on the provider side of health care — e.g., physicians, clinics, hospitals, biomed manfufacturers, pharma, insurors, etc — claim to be losing money and need higher prices or they will withdraw from their respective spaces of operation. Yet, somehow, they’re all going to be thrilled to take less money under the Beneficent Natural Laws and Invisible Guiding Hand of the “competitive free market” as we “reduce health care spending.”
This short article underscores the sole selling point for the Democrats at least since Clinton time: We kill, maim, rape you – but less than that other guy. OMG, you cannot allow that other guy to win, he’ll kill you more!
The argument is actually quite compelling – undeniable even – if we grant one extra hidden premise: TINA. Another way of expressing this, in imperitive mode: you must believe in the system. (Cue red baiting and brown baiting, both, not inconsequentially, specialties of the otherwise rather feckless Hillary Clinton camp.)
I reckon we’ll all be dead soon enough, one way or another. Sadly, that Grim Visitor who brooketh no protest shall visit many of us sooner than we would have anticipated.
That sounds rad and stuff, until we realize we’re talking about our children. (I’m a family man – soft like that. I’m seeing the future with clarity, and I want to turn away…)
If I did the math right and if results have matched the projections from the study Joe Firestone was using in “Neoliberalism Kills,” Obamacare has killed about 269,000 people from its initial implementation up to the end of 2016, relative to the Medicare for All alternative they could have passed and implemented instead at the beginning of the Obama administration.
So, through to 2026, that’s 589,000 killed by Obamacare even if it’s preserved now, and a little over 800,000 if it’s replaced by the AHCA.
But of course if they’d done Medicare for All 8 years ago there’d be no talk about an AHCA now in the first place (or, for that matter, a Trump administration at all), so I’m just going to go ahead and attribute all 800,000 of the fatalities under that scenario to Obamacare.
President Turns Out I’m Really Good At Killing People sure wasn’t exaggerating when he made that observation.
Any chance o prosecuting Obama for Class War Crimes as well as actual War Crimes? Just asking?
Thank you, nobody for remembering that reference. In an earlier comment which I don’t see posted yet. I referenced my recent update and extension of those projections this past April 10th. That post projects through 2024. It has much more context than Matt’s post above, but not as neat a presentation in terms of an interactive graph. Anyway, I used a different fatality ratio than Matt, 1 in 781 fatalities, rather than 1 in 830. I explain why in my post, and also survey other possible ratios that might have been used. Total fatality figures are quite sensitive to the ratio used, so you may want to read my post if you found this one interesting.
We’ll need to extend the legal construct behind the Good-Samaritan Laws in order to prosecute public officials for failure to prevent the unnecessary deaths at issue. There could be a few sticking points; such as, failure to prevent the election of public officials who fail to prevent unnecessary deaths–just to name one.