By Lambert Strether of Corrente.
Patient readers, I am buffeted by two enormous firehoses of information: the 2024 election, and Covid. While I do try to present the most important Covid information, there’s so much of it just now that important material gets left on the cutting room floor. So think of this post as my “director’s cut” on Covid; the three-and-a-half hour version as opposed to the ninety-minute one that made it into the theatres. (I went through the links from trusted sources I’d flagged to read since March 1 (!), and opened up about 200 tabs, so even the verbose post you are about to read is selective.)
Before I begin: (1) Covid is not “over”; mass infection from the pandemic continues. (2) Covid is airborne. If you’re feeling the urge right now to dispute either proposition in comments, let me advise you: don’t.
What follows is a compendium of worthwhile material I simply haven’t been able to get to, grouped into the following categories: #CovidIsAirborne, Non-Pharmaceutical Interventions (NPIs), Testing, Sequelae, Immune Dysregulation, Children, Social Norming, Gaslighting, Official Maleficence, and Eugenics. Feel free to skip to the category most interesting to you!
#CovidIsAirborne
“Bus Riding as Amplification Mechanism for SARS-CoV-2 Transmission, Germany, 2021” [Emerging Infectious Diseases, CDC]. From the Abstract: “A phylogenetically unique strain and epidemiologic analyses provided a link between air travelers and cases among bus company staff, schoolchildren, other bus passengers, and their respective household members. The attack rate among bus-riding children at 1 school was ≈4 times higher than among children not taking a bus to that school. The outbreak exemplifies how an airborne agent may be transmitted effectively through (multiple) short (<20 minutes) public transport journeys and may rapidly affect many persons.” • More on the quarantine-breaking driver from CIDRAP here. The first epidemiogical study on airborne tranmssion that I spotted was also from a bus, in March 2020 (from the South China Morning Post, complete with seating chart). Which would make the CDC about — [allow me to break out my calculator] — 2024 – 2020 = 4 years late. Still, it’s always good to add to the literature!
“COVID-19 outbreak at a residential apartment building in Northern Ontario, Canada” (accepted manuscript) [Epidemiology and Infection]. “A case-control study examined building-specific exposures and resident behaviours that may have increased the odds of being a case. A professional engineer assessed the building’s heating, ventilation, and air conditioning systems. Whole genome sequencing and an in-depth genomic analysis were performed. Forty-five outbreak confirmed cases were identified. From the case-control study, being on the upper floors (OR: 10.4; 95% CI: 1.63-66.9) or within three adjacent vertical lines (OR: 28.3; 3.57-225) were both significantly associated with being a case of COVID-19, after adjusting for age. There were no significant differences in reported behaviours, use of shared spaces, or precautions taken between cases and controls. Assessment of the building’s ventilation found uncontrolled air leakage between apartment units. A single genomic cluster was identified, where most sequences were identical to one another. Findings from the multiple components of this investigation are suggestive of aerosol transmission between units.” • Amoy Gardens all over again.
“Molecular detection of SARS-CoV-2 and other respiratory viruses in saliva and classroom air: a two winters tale” [Clinical Microbiology and Infection]. From the Abstract: “We analyze saliva, air, and air cleaner filter samples from studies conducted in two Swiss secondary schools (age 14-17 years) over seven weeks during the winters of 2021/22 and 2022/23. Two bioaerosol sampling devices and HEPA filters from air cleaners were used to collect airborne virus particles in five classrooms…. The weekly probability of airborne detection was 34%… for SARS-CoV-2 and 10%… for other respiratory viruses. There was a distinct shift in the distribution of respiratory viruses from SARS-CoV-2 during the Omicron wave to other respiratory viruses one year later. SARS-CoV-2 is more likely to be detected in the air than other endemic respiratory viruses, possibly reflecting differences in viral characteristics and the composition of virus-carrying particles that facilitate airborne long-range transmission.”
If only SARS-CoV-2 were visible:
1️⃣ Last Monday, my family was briefly exposed to a symptomatic person who had tested negative on a RAT. When I realized they were symptomatic, I asked them to leave as a precaution, and immediately refreshed the air via doors and windows open. They tested + the next day.
2/
— C Pita 🇺🇦🌻 (@CPita3) December 28, 2021
“Insurance Case Hinges on Whether Covid Virus Damages Property” [Bloomberg]. “Chubb Limited-owned Vigilant Insurance Co. argues because ‘the mere temporary presence of an easily removed foreign substance—a water spill, a wafting odor, or microscopic aerosolized droplets—does not distinctly and demonstrably alter the property itself, it does not qualify as direct physical damage or loss under the plain policy language implemented in California’s longstanding’ standard. ‘Our policy doesn’t include [treating] property as air,’ said Vigilant attorney Jonathan D. Hacker with O’Melveny & Myers LLP. ‘It’s not even insurable property.'” • Oh.
NPIs: Ventilation and Filtration
“Ventilation Can Reduce Exposure to Respiratory Viruses in Indoor Spaces” [National Center for Immunization and Respiratory Diseases, CDC]. “Good ventilation can help safeguard our health by reducing our exposure to respiratory viruses. People can still get sick after ventilating a space, so it is important to use ventilation as one part of a multi-layered approach to protect ourselves against getting sick from respiratory viruses…. Respiratory viruses primarily spread in the air between people. The fewer viruses in the air, the better. Improving ventilation can help you reduce virus levels in your home and reduce the chances that the virus will spread.” • Better late than never. Commentary:
More genius from this account… https://t.co/2YDI2PVgDe
— Michael R. Hicks, COVID Dissident (@Michael59503746) March 23, 2024
Maybe CDC’s HICPAC should read this.
“Ventilation Should Be A Larger Focus In Our Fight Against Covid-19” [Judy Stone, Forbes]. A good roundup, including this: “Richard Corsi, co-inventor with Jim Rosenthal of the Corsi-Rosenthal box, a DIY air filter, and now dean of engineering at the University of California Davis, also helped address the issue of cost and benefits with figures that are easier to relate to. Corsi said, “We could put a CR Box in EVERY public school classroom in the United States at a cost of $160M/year. That’s less than one Venti American coffee per student per year (or 0.024% of the average cost of educating a child each year in the US). In doing this calculation I have used a bulk discount for filters, which lowers the cost of a CR box by about 35%. We could do the same with HEPA air cleaners at about twice the price – 1 Grande Mocha Cookie Crumble Frappuccino per student per year.” He estimated the costs would be a bit higher for offices but still relatively low cost, given improved employee performance. The best thing we can do to reduce risk? Let in fresh air.'” • On CR boxes, see NC here and here.
NPIs: Masking
Alert reader Propertius writes:
I’m still masking everywhere, too. It’s not a matter of “fear of getting COVID again” because I’ve *never* had it. Not once, even though most of my friends and acquaintances are on their third or fourth cases. I haven’t gotten anything else since January, 2020, either. Four years with no COVID, no influenza, no colds. Being sick is a really miserable experience and I’m delighted I haven’t gone through that since the pandemic first began. It’s not a matter of “fear”. Instead, it’s a matter of simple joy in not being ill. In my view, risking easily avoidable illness isn’t “brave”, it’s just stupid.
“San Antonio hospital could have an answer to the PPE crisis– elastomeric masks” [KENS5]. From 2020, but ever green. “‘We are the only center in the U.S. which uses elastomeric masks routinely,’ [Medical Director] Dr. Annie Kizilbash said… She says the Elastomeric North 7700 Respirator is Hypoallergenic and made 100 percent of silicon and the center has 130 of these masks being routinely used…. The hospital specializes in treating tuberculosis patients. Dr. Kizilbash says the Elastomeric is highly effective against airborne diseases such as Tuberculosis. She says the center has used them since 1996 and not once did an employee test positive for TB. ‘They use P100 filters. What that means is that they’re oil proof and the 100 part means they’re 99.97% effective against airborne particles which is more so than the N95 which is 95% effective.'” • Today being World Tuberculosis Day.
“Why wear a mask to a protest?” [The Gauntlet]. This concept is, apparently, controversial in some large fraction of the putative left. The deck says it all. “Why spread illness when you could not do that?”
Masks as fashion items (a hobby-horse of mine):
My source is Mask Lab in the US! https://t.co/kcvw4DGV7Z
— Abby du Nord (@abbyobenchain) March 2, 2024
Readers will recall I occcasionally mutter about about clip art that represents masks with “Baggy Blues” rather than N95s (making commericial artists and art directors into propagandists for ineffective NPIs). So what does Adobe go and do?
Adobe removed all of the respirator, SARS, COVID, and mask shapes I had been using to make awareness graphics.
So now I need a new program
It has to work on my phone so its accessible and can't be Canva because I am anti genocide.— Gwen B. with LC 𓅟 (@PenGwenWithLC) March 19, 2024
NPIs: UV
“222 nm far-UVC light markedly reduces the level of infectious airborne virus in an occupied room” [Nature]. Mouse study using aerosolized murine norovirus (MNV) as a proxy for SARS-CoV-2. From the Conclusion: “In summary, we have shown for the first time that far-UVC light, operating well within current regulatory limits, is able to produce major reductions in the level of airborne viruses in an occupied indoor location. However, unlike controlled laboratory studies, uncertainties related to airflow pattern, residence time, and actual exposure dose experienced by the collected virus introduces uncertainty into the inactivation estimates. Whole-room disinfection with far-UVC is an emerging intervention for pandemic and epidemic control that has the potential to become part of the layered strategic approach to minimize transmission of airborne pathogens in occupied indoor spaces, including ventilation and filtration and, where appropriate, masks and physical distancing.” • Flagged and discussed by Naomi Wu. And speaking of UV:
Left behind in the giant movie studio stage from when COVID protocols existed are at least eight $2,565MSRP top of the line industrial air purifiers including UVlight filter in addition to HEPA. Sitting unused, forgotten.
— thomas 🛠 (@t_NYC) March 22, 2024
Testing
Without testing, we’re back to proxies for infection. Like ambulance sirens:
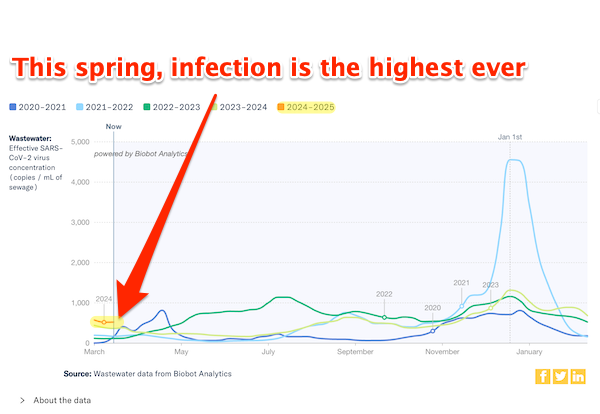
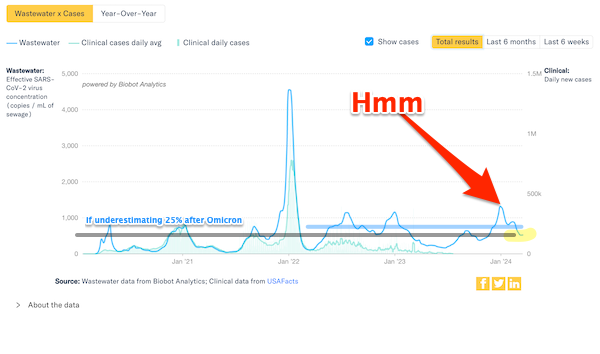
COVID-19 wastewater in NYC is high. https://t.co/PCd9zHYtbI pic.twitter.com/gXvHxIrLEv
— Myra Batchelder (@myrabatchelder) March 18, 2024
“Will Americans Ever Get a Combination Rapid Test for COVID, Flu, and RSV?” [Very Well Health]. “The COVID-19 pandemic made it commonplace to do an at-home rapid test to diagnose whether winter respiratory symptoms were from the virus. While getting a positive test in just a few minutes can solve the mystery, what if it’s not COVID? Outside of the United States, rapid tests exist for COVID as well as the other primary culprits for cold-weather respiratory symptoms: the flu and RSV. The combination tests are already available in Europe and Australia.” • The United States is not a serious country:
Post by @steeletalksView on Threads
Sequelae: Cognition
“Accelerated brain age in young to early middle-aged adults after mild to moderate COVID-19 infection” (preprint) [medRxiv]. From the Abstract: “Cognitive decline is a common adverse effect of the Coronavirus Disease of 2019 (COVID-19), particularly in the post-acute disease phase. The mechanisms of cognitive impairment after COVID-19 (COGVID) remain unclear, but neuroimaging studies provide evidence of brain changes, many that are associated with aging. Therefore, we calculated Brain Age Gap (BAG), which is the difference between brain age and chronological age, in a cohort of 25 mild to moderate COVID-19 survivors (did not experience breathlessness, pneumonia, or respiratory/organ failure) and 24 non-infected controls (mean age = 30 +/− 8) using magnetic resonance imaging (MRI). BAG was significantly higher in the COVID-19 group (F = 4.22, p = 0.046) by 2.65 years. Additionally, 80% of the COVID-19 group demonstrated an accelerated BAG compared to 13% in the control group (X2 = 20.0, p < 0.001). Accelerated BAG was significantly correlated with lower cognitive function (p < 0.041). ”
“Blood Markers Show Neural Consequences of LongCOVID-19” [Cells]. N = 33. From the Conclusion: “This study reports differentially expressed peripheral markers of inflammation and stress after SARS-CoV-2 infection between healthy pre-pandemic controls, people recovered from COVID-19 and neuroLongCOVID-19 subjects. Neurotoxic proteins associated with neurodegeneration were identified from neuronal enriched EVs that differed between the three groups. One or more of the proteins identified in this study have also been shown in other neurological disorders (e.g., AD, HIV-associated neurocognitive disorder, Parkinson’s disease, epilepsy, multiple sclerosis, Guillain–Barre syndrome, amyotrophic lateral sclerosis) with other etiologies (bacteria, fungus, other viruses), suggesting common pathological mechanisms. It remains to be seen, perhaps with the use of machine learning algorithms, whether our specific panel of combined proteins uniquely identifies neuroLongCOVID-19 and, thus, may serve as biomarkers for this disease.”
Sequelae: Heart
“The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications” [Heart]. From the Abtract: “We conducted a staggered cohort study based on national vaccination campaigns using electronic health records from the UK, Spain and Estonia. Vaccine rollout was grouped into four stages with predefined enrolment periods. Each stage included all individuals eligible for vaccination, with no previous SARS-CoV-2 infection or COVID-19 vaccine at the start date…. The study included 10.17 million vaccinated and 10.39 million unvaccinated people….. COVID-19 vaccination reduced the risk of post-COVID-19 cardiac and thromboembolic outcomes. These effects were more pronounced for acute COVID-19 outcomes, consistent with known reductions in disease severity following breakthrough versus unvaccinated SARS-CoV-2 infection.” • I would want the vaccine types and brands separated out; MRNA vs. killed virus, etc.
Sequelae: Cancer
“US -Death Trends for Neoplasms ICD codes: C00-D48, Ages 15-44” (preprint) [ResearchGate]. From the Abstract: “In this study we investigate trends in death rates from neoplasms (ICD-10 codes C00-D48) in the USA using crude data from the CDC (Centers for Disease Control and Prevention). We limit our investigation to individuals aged 15 to 44 and for the period of 2010 to 2022…. Using different metrics, we compare mortality trends due to neoplasms before the COVID-19 pandemic with the pandemic period. We show a rise in excess mortality from neoplasms reported as underlying cause of death, which started in 2020 (1.7%) and accelerated substantially in 2021 (5.6%) and 2022 (7.9%). The increase in excess mortality in both 2021 (Z-score of 11.8) and 2022 (Z-score of 16.5) are highly statistically significant (extreme events)…. The results indicate that from 2021 a novel phenomenon leading to increased neoplasm deaths appears to be present in individuals aged 15 to 44 in the US.
Sequelae: Long Covid
“Survey Finds Nearly 7% Of American Adults Have Long Covid Symptoms” [Kaiser Health News]. A roundup of coverage on this CDC “Household Pulse” (if any) study.
“Long COVID and Post-COVID Conditions” [Pandemic Patients]. From the introductory paragraphs: “For many people, being exposed to SARS-CoV-2 (the virus that causes COVID-19) results in illness characterized by mild symptoms, resolving in a matter of days or weeks. In fact, research has found that 30-60% of COVID-19 cases may be entirely asymptomatic (Shang et al., 2022; Wang et al., 2023). However, that is not the only potential outcome, and each infection is a new opportunity for long-term symptoms to develop (Bowe et al., 2022). In fact, some people experience severe, debilitating symptoms that may last for several years and may not improve over time (Fernandez-de-las-Peñas et al., 2023). Other people recover from COVID-19, but as a result of the infection, they are now vulnerable to many types of health conditions, known as “post-COVID conditions,” or “PCCs” (Fernandez-de-las-Peñas et al., 2023; Xie et al., 2023). These conditions affect nearly every organ in the body and range from benign to life-threatening (Bowe et al., 2022; D’Isabel et al., 2023; Zhao et al., 2023; Novak et al., 2022; Fernandez-de-las-Peñas et al., 2023; Xie et al., 2023; Peter et al., 2022; Abbasi, 2022; Ormiston et al., 2022; Ma et al., 2023). However, there is no way to know who will be susceptible to a particular condition until it manifests…. [T]he damage done by COVID-19 is cumulative (Bowe et al., 2022). Even someone who recovers from an asymptomatic (Ma et al., 2023) or mild case (Novak et al., 2022) of COVID-19 is at risk of developing one or more PCCs.” • This is an enormous document, and I can’t evaluate everything in it. Perhaps some readers will be motivated to look into it and report back.
“An ER doctor’s experience with long COVID – ‘My symptoms seemed endless'” [Hospital News]. “I didn’t get COVID at work. I got it from my junior kindergarten-aged son after kissing him goodnight in between the stairway banisters…. At the time, I remember feeling lucky to be fully vaccinated, and anticipated a full recovery. I returned to work on day 11 after testing positive for COVID, fatigued, but otherwise fine. I was training for a 10-kilometre run, and on day 16 tried to go for a jog. I couldn’t get down the street. I walked home. ‘That’s odd.’ I thought, believing it was just a premature return to sport. I worked two overnight shifts in the ED that weekend. By day 21, I was suddenly, terrifyingly, sick with something that felt altogether very new. That’s when my life changed forever. After that, long COVID took over my life. My symptoms seemed endless.” But: “Many people ask me what I want the public and physicians to know about long COVID. I think the first is that ‘the tests are not normal’ – we are just not ordering the right tests. Every study of long haulers shows unbelievable pathology: immune dysregulation, mitochondrial dysfunction, neuroinflammation, brain damage, vascular damage, gut dysbiosis, poor perfusion of the brain, lungs and other organs. We just don’t have an easily accessible biomarker yet.” Thanks, NIH! And: “The second thing is that while there are no approved treatments for long COVID yet, there IS hope, and there are treatments that help! Antihistamines, antidepressants for neuroinflammation, aggressive treatment of autonomic dysfunction, or POTS, resting and pacing for post-exertional malaise – these things can help. The third is that the best way to prevent long COVID is to avoid getting COVID. I use Can95 masks, nasal sprays and HEPA filters… And finally, we need a rapid acceleration of double-blinded, placebo-controlled, randomized clinical trials.”• Again, thanks NIH, which blew a billion dollars on Long Covid without spending on nickel on the search for biomarkers.
Sequelae: Versus Flu
“Long-term outcomes following hospital admission for COVID-19 versus seasonal influenza: a cohort study” [The Lancet]. N = 10 ,985. From the Abstract: “Although rates of death and adverse health outcomes following hospital admission for either seasonal influenza or COVID-19 are high, this comparative analysis shows that hospital admission for COVID-19 was associated with higher long-term risks of death and adverse health outcomes in nearly every organ system (except for the pulmonary system) and significant cumulative excess [disability-adjusted life-years (DALYs)] than hospital admission for seasonal influenza.” • So please don’t let anyone tell you “it’s just the flu.” Influenza is bad, and Covid is much worse.
“The Covid-19 pandemic killed off one strain of the flu, and that will change the next vaccines” [CNN]. “Yamagata viruses were in decline before the pandemic, and all the precautions that helped people avoid Covid-19 – including masking, staying at home and better ventilation – appear to have finished them off. They haven’t been detected in testing since March 2020.” • Lockdowns aren’t the only reason people might “stay home,” but they were certainly one reason. So the headline is deceptive: “The pandemic” didn’t kill off anything. NPIs did. A further exchange on this topic:
When I pointed out the huge drop in influenza mortality during the pandemic, @DrJBhattacharya, liked this post suggesting "viral interference" explained it. There is only one problem with this and that is the total number of RESPIRATORY INFECTIONS OF ALL KINDS DROPPED… pic.twitter.com/Ps5aAWIWHD
— Bob Morris, MD, PhD (@rdmorris) March 8, 2024
Sequelae: Reproduction
“SARS-CoV-2 infection negatively impacts on the quality of embryos by delaying early embryonic development” (preprint) [medRxiv]. From the Abstract: “Sixty-five SARS-CoV-2 infected infertile patients and 258 controls were involved in this study… SARS-CoV-2 infection reduced the number of oocytes and high-quality embryos on day 3. It delays the early embryonic development from the six-cell stage to blastocyst stage and has a negative impact on the quality of embryos.”
“Updates in the pathophysiology of COVID-19 infection in male reproductive and sexual health: a literature review” [Frontiers in Endrocrinology]. From the Abstract: “We conducted a literature review focusing on the possible pathophysiology by which severe acute respiratory syndrome corona virus 2 (SARS-CoV-2) affects men’s sexual and reproductive systems…. Findings revealed the adverse consequences of SARS-CoV-2 at cellular and organ levels on the male genital tract. However, the reported data are still controversial.”
Immune Dysregulation
“More attention should be paid to Omicron-associated sepsis: a multicenter retrospective study in south China” [Journal of Thoracic Disease]. N = 299. From the Abstract: ” This multicenter retrospective study included adults hospitalized with confirmed SARS-CoV-2 infection across six tertiary hospitals in Guangzhou, China from November 2022 to January 2023. The Sequential Organ Failure Assessment (SOFA) score and its components were calculated at hospital admission to identify sepsis…. In our study, 147 patients (64.19%) were identified as having sepsis upon hospital admission… A considerable proportion of patients infected with Omicron present with sepsis upon hospital admission, which is associated with a poorer prognosis. Therefore, early recognition of viral sepsis by evaluation of the SOFA score in hospitalized coronavirus disease 2019 patients is crucial.” • Yikes. China only?
“Shingles cases are increasing in New South Wales. Experts say COVID might be why” [ABC Australia]. “In 2022, a paper published by Oxford University Press reported that COVID was linked to an increased risk of shingles in patients over 50. Coincidentally, some data suggests shingles cases have increased across age groups in parts of the country since 2020…. But, pointing to the 2022 study of COVID patients being 15 per cent more likely to develop shingles, [Tony Cunningham, director of Westmead Institute’s Centre for Virus Research] said an explanation could be the immune system. One factor for an increased likelihood of shingles is reduced function of the immune system, the same reason why shingles is more common in older people, Professor Cunningham said. Separately, one side effect of COVID can also be reduced function of our immune system. ‘We do know that COVID can disturb immunity, particularly the severe causes where you can get variable responses to COVID,’ Professor Cunningham said. ‘That would be my best bet in the absence of clear evidence.'”
“World’s most deadly infection’ can be transmitted simply by breathing, scientists warn – as cases rise” [The Sun]. “Until now, healthcare experts thought TB germs were transmitted via coughing, laughing or speaking, singing or sneezing. But a new study has found that four in five people testing positive for the killer bug don’t suffer from a cough – previously thought to be a key symptom of TB. However, even those who don’t have a cough carry the infectious disease in their spit, which can be spewed into the air when someone talks or breathes, they found. This means people can pick up the infection just by breathing near someone who has the bug but isn’t showing any obvious signs, they said. ‘A persistent cough is often the entry point for a diagnosis,’ study author Professor Frank Cobelens of Global Health at Amsterdam University Medical Center said. ‘But if 80 per cent of those with TB don’t have [a cough], then it means that a diagnosis will happen later, possibly after the infection has already been transmitted to many others, or not at all,’ he added.” And: “Cases of the Victorian disease increased by over 10 per cent last year, according to the UK Health Security Agency – up from 4,380 in 2022 to 4,850 in 2023.” But: “Health chiefs are scrambling to ‘investigate the reasons’ behind this sudden infection rise.” • ‘Tis a mystery!
Children
“Lockdowns had an impact on gut microbes and allergies in newborns, new research reveals” [Science Daily]. “The findings highlighted gut health benefits for ‘pandemic babies’ arising from the unique environment of lockdown including lower rates of infection and consequent antibiotic use, and increased duration of breastfeeding. The newborns were found to have more of the beneficial microbes acquired after birth from their mothers. These maternal microbes could be playing a protective role against allergic diseases.” • Lol.
Social Norming
Some of the people responding seem angry:
Fascinating how wearing masks (or not) can be contagious.
When boarding my plane, I had on my mask. Several people upon noticing me, also retrieved theirs and put them on. Seems seeing others wearing masks provides a social cue or reassurance to do the same. 😷👍🏽 pic.twitter.com/ywEGgGGfZB
— Jerome Adams (@JeromeAdamsMD) March 1, 2024
I don’t know how in the world Trump’s Surgeon General became a beacon of sanity, but here we are (no, Adams isn’t perfect; but at least, unlike Biden’s Vivek Murthy, he’s not wandering around prattling about a loneliness epidemic after Biden managed to infect all our public spaces with an asymptomatic airborne biohazard).
“Always in a 1-on-1 setting”:
"My field necessitates high risk contact. In conversations with colleagues there are starting to be louder and louder whispers (always 1 on 1, never a group), about Covid having disastrous long term impacts on our health." pic.twitter.com/cZYzl111EG
— Nate Bear (@NateB_Panic) March 20, 2024
More reaction to that horrid NPR story:
And it's not enough for them to feel like just good people. They need to feel like most moral, most reasonable people in the room at all times.
— lizwhatsherface (@RealGayArbys) March 11, 2024
Not sure what the equivalent armchair psychology for conservatives would be (maybe if they understand that NPIs. as one layer in a multilayer strategy, would replace our current vax-only strategy?)
More armchair psychology (not that there’s anything wrong with that):
#1 – Denial – Pretending a problem does not exist to provide artificial relief from anxiety.
Examples:
“During COVID” or “During the pandemic” (past tense)
“The pandemic is over”
“Covid is mild”
“It’s gotten milder”
“Covid is now like a cold or the flu”
“Masks don’t work… pic.twitter.com/W2LbrMyrZC
— Mike Hoerger, PhD MSCR MBA (@michael_hoerger) December 20, 2023
Here is the ThreadReader.app version.
Gaslighting
So many, many examples of The Semmelweis Reflex:
Next time you're feeling #gaslit, remember Alton Ochsner was subject to "ridicule and #vituperative attacks" for his advocacy linking smoking to the "rare" condition of lung cancer. pic.twitter.com/T5O0J2WGDW
— Mike Hoerger, PhD MSCR MBA (@michael_hoerger) March 23, 2024
“Experts Can’t Agree If We’re Still in a Pandemic” [Time]. “But are we still a pandemic? No one seems to know for sure. When I asked Dr. Mandy Cohen, director of the U.S. Centers for Disease Control and Prevention (CDC), she didn’t give a direct answer. ‘Rather than getting caught up in the semantics of it,’ she says, people should feel confident that ‘we are outside of the emergency [phase]. But I don’t want folks to forget that COVID is still here and still poses a risk.'” Which is why Mandy still masks. Oh, wait…. More: “Dr. Robert Wachter, chair of medicine at the University of California, San Francisco, has stopped using the word ‘pandemic,’ which he says was a ‘shorthand way to convey to the public’ that COVID-19 constituted a worldwide emergency that required a global shift in behavior. But calling it a pandemic now ‘just doesn’t feel right,’ he says. In his opinion, we’ve been out of the pandemic phase for about a year, given the widespread availability of tests, treatments, and vaccines.” And mass infection. Maybe Wachter has a 23-step procedure for determining vibes? “So what’s the word to use now? Experts interviewed for this story were hesitant to pick one. ‘We really don’t have the language for things that are somewhere between flus and cold viruses and pandemics,’ [Dr. Jonathan Quick, an adjunct professor at the Duke Global Health Institute] says.'” • Idea: How about “pandemic”?
Official Maleficence
“Covid no longer controls our lives.” —Joe Biden. Commentary:
One thing I wish more people knew about the US economic recovery from the *pandemic-induced* recession is that far more working age adults died of covid from Mar2021-Feb2022 (146,896) than Mar2020-Feb2021 (104,042) — despite improved knowledge, vaccines, and Biden as president pic.twitter.com/2plsQsL9I3
— wsbgnl (@wsbgnl) March 7, 2024
Should somebody check in on the Infectious Diseases Society of America?
Yep, confirmed. That utter wanker @CarlosdelRio7 is the new president of @IDSAInfo. Carlos is the shit bird from Delta that got the original 10 days lowered to 5 days, which resulted in the greatest amount of LongCovid by any one person in history.
Fuck you, Carlos. https://t.co/DjyNaAwPyP pic.twitter.com/qA1wBQffmP
— Lazarus Long (@LazarusLong13) March 3, 2024
Del Rio:
Bottom signature on the left… Carlos del Rio. pic.twitter.com/ktJi7CW4VJ
— Taylor Whitney (@taylorwhitney88) March 3, 2024
Ka-ching!
“Critical Care Nurses’ Moral Resilience, Moral Injury, Institutional Betrayal, and Traumatic Stress After COVID-19” [American Journal of Critical Care]. N = 121, online survey. From the Abstract: “Traumatic stress and moral injury may contribute to burnout, but their relationship to institutional betrayal and moral resilience is poorly understood, leaving risk and protective factors understudied…. Of participating nurses, 71.5% reported significant moral injury symptoms and/or traumatic stress. Both moral injury symptoms and traumatic stress were associated with burnout. Regression models showed that institutional betrayal was associated with increased likelihood of traumatic stress and moral injury…. [S]ystem factors (eg, institutional betrayal) must also be addressed systemically rather than relying on individual-level interventions to address nurses’ needs.”
And speaking of institutional betrayal:
How Mandy Cohen would have gotten people to follow CDC Guidance on indoor smoking in the 90's: pic.twitter.com/22COif6ogJ
— Love thy neighbor: wear an N95😷 (@CCSDMaskUp) March 2, 2024
It’s been a long, long time since I agreed with Imani Gandy about anything:
The CDC now recommends that you quote go fuck yourself end quote https://t.co/wxcZwCZ7qo
— Imani Gandy (Orca’s Version) ⚓️ (@AngryBlackLady) March 2, 2024
And the WHO:
Look at this.
The @WHO corrects an earlier incorrect tweet via an ERRATUM tweet. So they CAN if they want to.
But somehow they REFUSE to write an erratum for the many “COVID-19 is NOT airborne” tweets that are still uncorrected and can still misinform the world.@gabbystern? https://t.co/ZN5IQf1Ip7
— Maarten De Cock (@mdc_martinus) March 1, 2024
Yes, this infamous (and false) post is still up, still doing damage;
FACT: #COVID19 is NOT airborne.
The #coronavirus is mainly transmitted through droplets generated when an infected person coughs, sneezes or speaks.
To protect yourself:
-keep 1m distance from others
-disinfect surfaces frequently
-wash/rub your 👐
-avoid touching your 👀👃👄 pic.twitter.com/fpkcpHAJx7— World Health Organization (WHO) (@WHO) March 28, 2020
And no Erratum. Funny thing.
Eugenics
“The Great Barrington Declaration Wasn’t a Plan For Public Health Officials. It Was a List of Absurd Demands of Them” [Science-Based Medicine]. “[L]et’s consider the plan to to ‘protect the vulnerable’, which was the pillar of the Great Barrington Declaration (GBD). How might we have accomplished this laudable goal? Though many people thought the best way to protect the vulnerable was to limit spread of COVID and vaccinate as many people as possible, the GBD claimed that by spreading the virus among hundreds of millions of unvaccinated, ‘not vulnerable’ Americans, herd immunity would arrive in 3-6 months, and the pandemic would be ‘naturally over.'” Obviously, that was a debacle, and therefor its proponents are still making bank, along with the neocons who got us unto the Iraq War, Larry Summers, and everyone else who’s wrong about everything. More: “A section of the GBD titled Protecting the Old and Other High-Risk Groups laid out their ‘plan’, which they called ‘focused protection.’ You should take 5 minutes and read it. It’s just 880-words long. Their answer to the question ‘How do we protect older people living at home?’ was only four sentences long… To pick just one example, the GBD wrote that ‘During high transmission times, older people should be offered home delivery of groceries and other essentials.’ That sounds nice, but it’s worth thinking seriously about this part of their ‘plan’ for a moment, something the authors of the GBD clearly did not do. Creating a program overnight to deliver fresh food and other essentials to tens of millions of seniors for months on end while the virus spread uncontrolled would not be an easy task…. In an interview from October 2021, a year after the publication of the GBD, Dr. Jay Bhattacharya sought to answer these questions by saying: “We could have offered free DoorDash to older people. I mean, yeah, it would depend on the community and the living circumstances. It would be a local thing, right?” This was obviously something Dr. Bhattacharya just thought of off the top of his head. The idea of millions of homebound seniors surviving off DoorDash for months on end is something a high school student might come up with.” • A high school master debater…
“”Poor, poor pitiful me”: Was Martin Kulldorff fired by Harvard?” [Respectful Insolence]. “If there is one narrative that is a constant among purveyors of misinformation, pseudoscience, quackery, and conspiracy theories, it’s a persecution narrative. In the realm of medicine and health, for instance, brave maverick doctors (like, for example, Martin Kulldorff) promoting antivaccine views and quackery, as well as the conspiracy theories that undergird them, always portray themselves as the hero persecuted by the medical and scientific establishment. While it is true that there have been physicians with alternative medical theories who were unfairly ostracized and persecuted but turned out to be right (e.g., Ignaz Semmelweis), in the vast majority of cases, the immortal words of Carl Sagan apply: ‘But the fact that some geniuses were laughed at does not imply that all who are laughed at are geniuses. They laughed at Columbus, they laughed at Fulton, they laughed at the Wright brothers. But they also laughed at Bozo the Clown.’… One of the GBD’s own flacks even (sort of) admitted it. It was always nothing more than an attempt to place a scientific veneer on a libertarian ‘open it all up’ strategy that would ignore the harms of the pandemic in favor of economics. It arguably did help achieve the cherished aim of anti-government activists and antivaxxers by, in essence, seriously degrading governments’ ability to institute public health measures during a pandemic. Through it all, going on for months and months, Kulldorff kept promising that ‘natural herd immunity’ was just 3-6 months away.” • And he’s still making bank, along with Bhattacharya and the other service providers at the house of ill fame that is Standord.
Ballastexistenzen (1):
Some people living with disabilities are worried about the stress of facing unexpected questions about whether they have considered #MAID. Some are drawing up cards, like the one below. Others suggest ID bracelets that say "No MAID".
"So many of us are worried about this,"… pic.twitter.com/stYL01SFbG— Avis Favaro (@Avis_Favaro) March 19, 2024
Ballastexistenzen (2):
Nothing quite sums up the hegemonic project of covid normalisation, and the total disregard for the lives of the vulnerable necessary to that project, like the last polio survivor living in an iron lung being killed by covid https://t.co/TxwWMvQEu4
— Nate Bear (@NateB_Panic) March 13, 2024
Conclusion
Unfortunately, I couldn’t splice everything together; there are only so many hours in the day. (Do note that the incredible volume of discourse on this topic is a hopeful sign; and some serious work is even breaking through to the national media, at long last.) Recently, many of you were highly complimentary of Naked Capitalism’s Covid coverage. However, I have been conscious of my own inability to get to every story and article that deserved to be covered. I hope this post makes up for that, in some measure. Let’s go save some lives!


{kind=link}
{kind=link}
I must to thank you in the way it counts though I am still estimating the chances my daughter might contact me needing more money else dire consequences result. Your posts on the many versions of Corona flu have been — a life-saver for me … most probably given my age. However, I have not been able to share your Wisdom with my near and dear for many reasons, though my reluctance is not one of those reasons. We most certainly live in most interesting times.
Great compilation, Lambert!
Many thanks.
Just curious as to why ““Ventilation Can Reduce Exposure to Respiratory Viruses in Indoor Spaces” appeared on the CDC website two days ago. Why now?
I am guessing that the CDC is applying a little CYA. Someone may feel a little sore from being savaged over their denial of airborne infection, so they are salving it with a PR release they can point to any time they are called out on their policy of denialism.
Limiting the liability, political and monetary, of all powerful organizations and persons for exposing the general public to Covid has been the substance of their policy — they are trying to get the spotlight off themselves.
My personal recent experience – I went to the dentist. Everyone except the receptionists were masked. EACH Dental-Station (there are 5) has an air filter machine – like this at Amazon – only much bigger. The room where root canals happen has a gigantic one.
I forgot to ask if they had many people catching COVID. But did say how happy I was to see these things. My hygienist said she wouldn’t work there without them.
It was very nice to see that some places are still taking things as seriously as they ever did. I know there could be more. The receptionists could be masked and the clients too. But this is WAY more attention than I’ve seen in years.
Hi Katiebird.
I went to the dentist last week in Ottawa, Ontario. I was relieved to find all the dentists, hygenists AND receptionists wore masks. My hygenist wore a 3M N95 Aura mask. My dentist only wore a baggy blue.
I have no idea how representative this is. Few people wear masks any more.
I spotted this quote, and as a card carrying [VISA] u.s.-ian — what is important in the u.s. !!! ?
“The combination tests are already available in Europe and Australia.” • The United States is not a serious country:”
NOT SERIOUS !!!!! ? The u.s. is a very serious country [Why so serious!?]. The most appropriate question to ask is what exactly, is the u.s. serious about?
And who exactly in the US is serious about what?
The CDC is very serious about deliberately on purpose infecting as many Americans with covid as many times as possible, over and over again, deliberately on purpose with malice aforethought. Or at least the political commissars who now own and run the CDC are very serious about that, and let each and every one of their captive scientists know it.
So lets not say the US is “not a serious country”. The US ( or at least those in authority here) is very serious about making the pandemic endemic and permanent, in order to kill as many vulnerable Americans as possible. On purpose.
Don’t tell me that isn’t “serious”.
Thank you, Lambert, for covering the many aspects of COVID over these last years. I’m quite sure you have saved lives as a result.
I did get COVID a year+ ago despite diligently practicing preventative measures. I don’t know how I caught it. I already had a serious medical condition so I suspect that my recent diagnosis of a related but much more aggressive condition may be the result of having COVID. Again, I don’t know. I was already living on borrowed time so I am at peace with this now, receiving ‘comfort measures’.
I do worry about people with Long COVID, especially children. What do their futures hold?
I am so sorry, Lena. Your strength is inspiring. And your comments very appreciated.
Worry not, there are very few of those cases (long Covid in children). The kids are alright.
It’s not even social democracy. It’s social insurance. The welfare state – and everytime I mention the phrase I have a well-developed tic which makes me explain that welfare is a good thing – provides a basic standard of living. This makes it so that working class people, those born without assets, can afford to live, while, from the employers’ perspective, makes it so that labor is affordable. If neither the employer nor the worker have to pay for infrastructure, education, and healthcare, then wages can be ‘competitive’, and capital does not leave the country in search of more exploitable workers. A welfare state is good for capitalism, basically.
Socialism would be workers owning the means of production, and the abolition of wage labor and commodity production.
Isn’t it quite the accomplishment, by the way, that Clinton was able to publicly shout about ‘ending welfare as we know it’? Think of the phrase “for the welfare of your child, make the right decision”, and reflect on this Orwellian turn.
If you were poking fun at the right-wing idea that socialism is when the government does anything except war, then I apologize! Even most right-wingers, however, can have their heartstrings tugged at when the ‘deserving poor’ suffer.
I believe you placed this comment on the wrong post. Otherwise, it looks like an attempt to thread-jack.
Are the Chubb and AIG insurance policies referenced first party Property policies or General Liability (third party) policies? No ‘contagious disease’ ‘microbial matter’ ‘naturally
If a Covid Round-Up were to become a permanent weekly feature . . . say . . . the Sunday Covid Roundup . …in the spirit of Tony Wikrent’s Weekly Wrap Up each Sunday over at Ian Welsh, would that attract a whole new tranche of readers to this blog? At least every Sunday?
Would it be worth trying it to find out?
And if it were tried, would there be things the readers here could do to try recruit other readers to come here at least every Sunday for a Sunday Covid Wrap-Up feature? What if readers got word of such a feature to the various primary sources of Covid truth and information who still keep posting over at TwitterX? Would they themselves begin referrencing the existence of such a feature at this blog and suggest to their readers that they come here and read it?
Thanks for this Lambert.
US -Death Trends for Neoplasms ICD codes: C00-D48, Ages 15-44
The first study I’ve seen that definitely shows an increase in cancer. That’s unfortunate. I haven’t wanted to simply accept anecdotal evidence on this, but here we have this study finally. This bodes ill.
I like to think I’ve avoided Covid thus far, but how would I know for sure?
I believe there is a blood test that can differentiate between antibodies to spike protein from being vaccinated and antibodies to other viral elements that are the result of infection.
This is spectacular; thanks so much!
My most hated trigger phrase these days is “post-pandemic”. Arrggghhh! Way too many journalists who ought to know better are using it, so I’ve started sending them snark-o-grams.
Today’s offender was the writer of an environmental newsletter on climate change. COVID denialism seems to be okey dokey though.
I cant be the only regular reader here (yes I have contributed, by check) who just rolls my eyes and shakes my head at everything covid on NC
If you don’t want to lose 3 IQ points and suffer 7 years of brain aging with each Covid infection, and risk getting Long Covid (incidence 38% with the third infection), that’s up to you. But some of us prefer to avoid that, and not harm the immunocompromised too.
lol
I’d say it’s a certainty that you’re not the only one. Many in links and water cooler post credulous and approving links to inane propaganda perpetuated by charlatans like Bhattacharya, and have done since 2020 (some used to get banned for it!). Said users conspicuously refuse to engage with detailed and substantive posts on the disease, such as this one, because their biases formed long ago and nothing will shift them. They are right. The MSM-afflicted other is wrong. Simple as. Much easier to lapse into a form of unthinking generic liberal paranoia (eg ‘plandemic’ and the many “they’re trying to take something away from us!!” vapidities downstream of it) and hewing to the accompanying just-so narratives that rationalise this worldview, than engage with complex reality, as Lambert does heroically and on a regular basis.
This worldview is in turn bolstered by altstream media celebrities like Taibbi, who see the obvious pecuniary benefit they stand to reap by working those fields, and pathetically and deliberately misunderstand this problem and regurgitate the propaganda line dictated by the pro-virus lobby. Their pivot from being “medicare for all” guys to “Sickness is good actually. Allow me to familiarise you with the (obviously and provably bullshit) works of Vinay Prasad and Jay Bhattacharya.” guys in just a few short years is grimly fascinating and marks them out, in my estimation, but as cynical Clintonian triangulators motivated purely by self-interest. But people simply love to gobble that shit up. Thus you occasionally see vacuous comment posts here that amount to digital belly-button lint like “hurrr I just see a post on covid here and roll my eyes”. Thoroughly depressing stuff!
Alas, reading this or any other blog is no guarantee of even rudimentary intelligence, let alone that much ballyhooed yet apparently very scantily understood concept, ‘critical thinking’.
“Everything” is a lot of things. Your lack of specificity speaks to failure of analysis.
If I’m exercised about anything, it’s not masking, but reckless (and continuing) GoF research.
Most definitely not the only one. Covid p0rn is rampant here.
I can’t spare the IQ points caused by repeat infections, so I am thrilled at the info Lambert tracks down. I can definitely see brain changes in people I know who have had covid. One change is that they stop caring about catching covid; it is like a switch has been flipped.
Thanks for this, Lambert. The persistence of and damage from COVID must be one of the most censored stories thus far in the 21st century.
Thanks for assembling this. I’ve been wondering about the possibility of putting together a one piece explainer using links from here. But as you know, it’s daunting. Anyone up for a collab effort using a wiki-like editing system? I can try to post a start as a water cooler comment if that’s ok with Lambert.
Great compilation Lambert. Thanks so much for your work.
It has been of great help to me in navigating through life with Covid. How sad that our public health people are not doing this.
Thanks for doing the hard yards in putting this post together. I certainly like this idea of a Director’s Cut as it brings so many elements and loose elements all under one roof though I have to say in reading it, it was like a night time walk through a haunted house. As for that ‘Shingles cases are increasing in New South Wales. Experts say COVID might be why’ article, it would explain why the past few years I have seeing at my GP’s waiting room advertisements for the shingles shot. In fact, when I had my annual exam recently they mentioned that they had dropped the age of those entitled to a free shingles shot and that now I was eligible. Hadn’t made the connection with shingles and Covid though.
There is a supreme irony in all this discussion about the present pandemic. All the authorities, especially the medical ones, ignored how it was spread as an aerosol and that it was time for everybody to go back to work. And now there is all this gaslighting that the pandemic is over and Covid is just like the flu, bro. This was all an effort to protect the 2019 economy so that all those stock portfolios would not have a sad. It was that simple. Now we know that Long Covid will constantly gut the economy and it is only going to get worse with each and every year.
But if the WHO, CDC, etc. had done the right thing back in 2020 and on by recognizing it as aerosol spread and mandating masks, ventilation and all the other measures that we know that work, that our economy would have been able to adapt. It would not have been the 2019 economy but it would have been one that was, oh I don’t know, actually sustainable going forward. But we did not take that path and now we have the worse of worlds. Heckuva job, that.
That’s not entirely true. While dissemination of the theory of airborne transmission early on would have been massively helpful, Australia and a few other countries solved the problem without an accurate theory of transmission, or public knowledge thereof. Thus Australia was mostly Covid free while faffing about with hand sanitiser and droplet masks (which probably helped as source control). They did this with a strong TTIQ protocol (Test, Trace, Isolate, Quarantine – you’ll remember the heroic contact tracing here in 2020 and 21, Kev). The key tactical fault – probably deliberate – was the USG (initiated under Trump, continued under Biden) pursuing the vax-only strategy and using inane Flatten The Curve tactics to shepherd in an acceptable amount of preventable deaths until such time as vaccines could be deployed. If the Operation Warp Speed money had been spent on innovations in testing rather than a vaccine (when it was known from early on that SARS would not be a vaccine-solvable problem) and the US adopted meaningful TTIQ (which it never did, but would have been massively influential due to its de facto status as the global hegemon), then Covid would be distantly in the rear view mirror by now.
One shouldn’t fall into the trap of thinking that Covid was and is inevitable, and indeed there is a hypothetical that repudiates the very idea: Say that SARS-CoV-3 (or 4, if you consider Omicron as SC3, which I tend to) emerged next week. And say among its properties were a transmissibility akin to Omicron and a Case Fatality Rate akin to MERS (~30%). Hardly probable but by no means biologically impossible. The consequences of the uncontained spread of such a disease speak for themselves. It wouldn’t just be Big Bad China that rediscovers the efficiencies of TTIQ in such a scenario.
Watching the data (what little remains available, and many thanks to Lambert for diligently collating and updating what is) suggests to me that Covid is not seasonal in the sense that the baseline of infection never really goes low enough. What DOES appear to be seasonal is human behaviour, especially with respect to the prevalence of indoor activities. So maybe the reliable rise of infections in the Fall (and sustained from November through March) is a reflection of changing human behaviour in the presence of a virus that is permanently circulating at some level.
If so, the refusal to widely communicate that Covid is airborne is an even more egregious and malicious failure on the part of public health officials and their political masters. And the refusal of those responsible for managing indoor air quality standards (with the connivance of those responsible for setting legal requirements for such standards) to take the steps necessary to create and sustain appropriate indoor air quality is downright eugenicist.
William Mitchell weighs in on Covid and labour supply, marvelling at the lack of an appropriate policy response:
https://billmitchell.org/blog/?p=61652
The “vaccine” is not a vaccine and those who received it should not be called “vaccinated.”
Whatever else, this is true.
“A phylogenetically unique strain and epidemiologic analyses provided a link between air travelers and cases among bus company staff, schoolchildren, other bus passengers, and their respective household members.”
I am in training to drive a small bus for a county in NY and drove with a senior driver Saturday. We went to an assisted living facility to pick up a resident and take him, and 3 other riders, to dialysis. We were told by the staff that the man had tested positive for Covid so they gave us a few surgical masks. Our boss was called and we were told to take him, to the DIALYSIS facility, but to wear masks and open a vent window! I wore my N-95 and opened ALL the vent windows but I won’t be doing that again. Unbelievable.
And the lucky patients at the DIALYSIS facility who get to spend a couple of hours with them as they get treatment. What are the odds that any were masked? Much less wearing N95s
Over the weekend I volunteered at an event for families of kids being treated for cancer, i.e. with suppressed immune systems. (I am blessed not to be in that demographic myself.) It’s the first time in a long time that I’ve seen masking taken moderately seriously. Among well over 100 people, virtually everybody masked. However, the instructions from the organizer only specified “high-quality masks (no cloth).” Baggy surgical masks were the dominant style among volunteers. Most of the patients and families wore KN95, but a few wore baggies too.
70 yo retired physician, take zinc and Vit. D3 daily, avoided all covid vaccines and boosters.
Wife and I have had two colds in 4 years, wife tested positive for covid on those two occasions.
I never got the test for covid, we were both sick for about 3 days, residual cough for a week.
For us covid has been a non-event.
Has your wife had a brain scan? Heart imaging? Even a single ca “mild” Covid results in a loss of IQ of ~3 points and seven years of brain aging.
no noticable residual effects on the brain or heart in either of us.
glad we didnt take the risks associated with the experimental vaccines though, they proved to be unsafe and ineffective as i suspected.
I’m with you on the vaccines and vitamin D. I got Covid early on and am still plagued by the auto-immune problems it triggered. A friend, who’s even older than I, and spends a lot of time on the same public transportation routes I do (one stops at a teaching hospital,) happened to be taking high doses of Vitamin D when covid hit our city in early 2020 and never had a symptom. It’s inconceivable that she wasn’t exposed to the virus, having never tried to avoid it. If our public health officials had recommended prevention at the end of 2019 (they knew what was coming by then,) a lot of us might be in better shape.
Thank you very much for this. It is greatly appreciated.
So the NIH losing a billion dollars is the heist of our era. Where did it go? Executives at NIH associated facilities and NIH senior staff should be in jail. This is a crime of incompetent and carelessness. I hope for a deep investigative report from a competent news outlet about this failure much like about CDC failure at original COVID tests. What a monstrosity.
I find Naked Capitalism’s coverage of COVID-19 puzzling, especially surprising given Lambert’s excellent climate change coverage, which I highly regard. What particularly stands out in this post is the inclusion of ‘The role of COVID-19 vaccines in preventing post-COVID-19 thromboembolic and cardiovascular complications’ study. It’s intriguing to consider how a vaccine, that was supposed to remain localized for a few days but later found in heart tissue months later, is touted for preventing cardiovascular complications.
I would love to see Naked Capitalism interview Vinay Prasad:
A flawed paper claims COVID19 vaccines prevent cardiovascular complications for a YEAR after the shot
This is from IM Doc:
> I would love to see Naked Capitalism interview Vinay Prasad:
We don’t do assignments. And we post what’s newsworthy, not what we agree with.
In any case, Prasad* would be the last person I’d amplify, or anyone from the eugenicist cesspit at the Brownstone Institute, for that matter. At some point I’ve got to deal with them, but not today. Today is my day to be kind.
NOTE * Prasad may have emitted a good take on one study. “Even a blind pig finds a truffle every so often.”