By Lambert Strether of Corrente.
I probably shouldn’t even tangle with David Cutler; he’s from Harvard, and he’s wicked smart. Anyhow. Also too, he advised the 2008 Obama Campaign on health care. But there were some things he said in this recent interview with PBS (and in his now famous 2010 letter to Larry Summers) that really ticked me off, and so I want to lay down a few markers. First, let’s look at two charts:
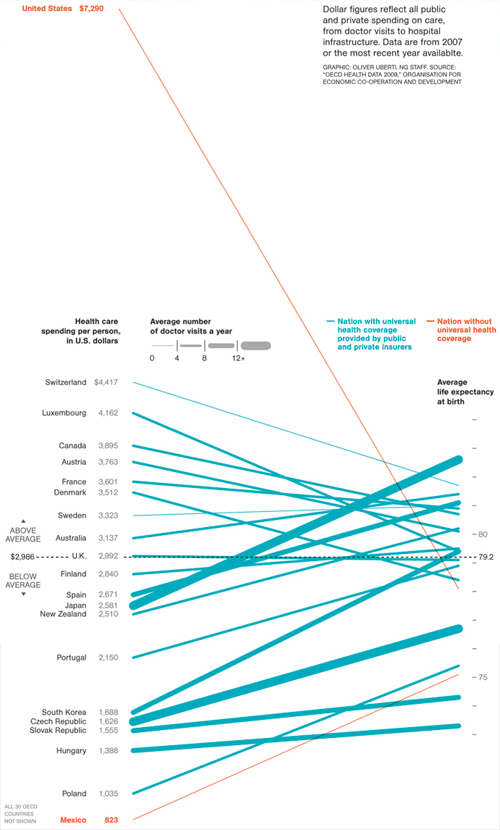
On the left, per capita spending. On the right, average life expectancy. The chart, from Michelle Andrews in National Geographic, shows that our health care system has costs are literally off the chart, and benefits — assuming life expectancy is a good measure of a health care system effectiveness — that are mediocre at best.[1]
Via Ezra Klein, who says:
This is serious pitchforks-and-torches stuff, if only people really understood it. … America may not be the best, but we’re not supposed to be the worst by such a large margin.
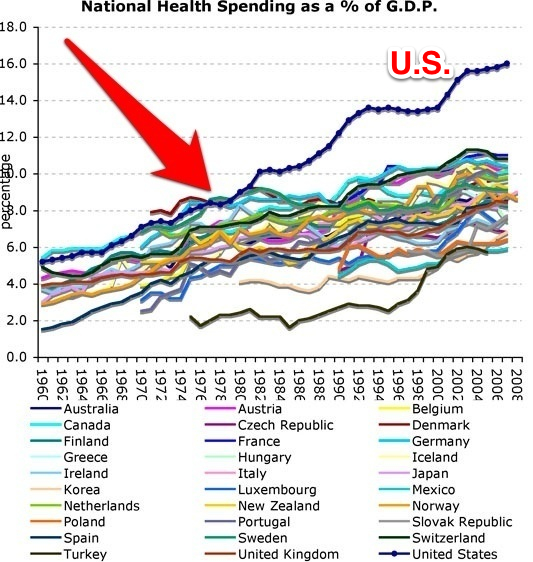
And here is our second chart[2]:
Via Catherine Rampell, who says:
[O]nce upon a time, it was more or less on par with its peers, and at various points even spent less of its G.D.P. on health care than some other countries (namely, Canada, Sweden, Denmark and Germany). …. Although you could quibble about the exact trajectories, it seems to have been in the late 1970s or early 1980s that America’s health care spending really broke from the pack.
Taken together, what do these two charts show? First, that there is at least one way that the United States is exceptional: flagrantly, floridly, off-the-charts exceptional. That is the cost of our health care system. It’s a wild outlier, globally. Second, there is another way the United States is exceptional: We are the only country that does not have universal health care[4]. We are also (as Andrews might have written, but did not) exceptional in the freedom we give the profit motive (“the market”) to operate in the health care system. All other countries have government regulate their health care delivery systems more tightly than we do, and many have single payer systems. Canada’s costs, for example, diverge from our own in the mid-70s, when they adopted a single payer system.
So those are the charts, and that is the background. Let’s turn to David Cutler. What does he have to say about our exceptionally high costs?
Paul Solman: Why does health care cost so much in America?
David Cutler: Let me give you three reasons why. The first one is because the administrative costs of running our health care system are astronomical. …. The second reason health care costs so much in America is that the U.S. spends more than other countries do on many of the same things. …. The third one is Americans receive more medical care than people do in other countries, not so much in terms of doctor visits, but if a person has a heart attack in the United States, they’re much more likely to get open heart surgery than they are in most other countries.
So far so good; I’ll take the reasons as read for the sake of the argument. And at this point — and maybe this is why I am where I am, and Cutler is where he is — I’d look at health care systems that accomplish what I want to accomplish, and try to adopt what they do, advocating for their approach if need be. Why reinvent the wheel? Not so Cutler:
David Cutler: [W]hat we’re doing is two things: one is on the demand side trying to make people smarter consumers, and the second is on the provider side, eliminating the monetary incentives to do more testing and procedures. Instead, let’s move to a system that says, “do what’s appropriate, make the patients better and you’ll get rewarded for it.”
(Oddly, or not, Cutler seem to regard reward as synonymous with monetary reward.) Notice, of course, that Cutler makes no effort whatever to compare or contrast ObamaCare’s approach with already proven systems (see the charts) that achieve his goals. No, he wants people to “shop.”
Paul Solman: So that will provide comparison shopping.
David Cutler: That’s on the demand side. Give people more skin in the game and give them the information so they can do real shopping.
Paul Solman: More skin in the game, meaning higher co-pays?
David Cutler: Higher co-pays.
I love that “skin in the game” trope, and so does Obama. Cutler, however, leaves out a detail: Under ObamaCare, the only people with skin in the game — their literal skin, I might add, since this is health care — are those who are not wealthy; the wealthy don’t have to worry about co-pays at all, or hospital concierges, or narrow networks, or balance billing, or any of that prole-type nonsense. Class warfare at its finest!
More importantly, note that Cutler’s approach to cost containment is experimental (“trying to make people”; “let’s move to”). In fact, Cutler says, quite explicitly, that from the cost containment perspective ObamaCare is an experiment in his famous 2010 memo:
For example, I recently met with the senior CMS staff about how all the new demonstration and pilot programs envisioned in the legislation might work. This is a crucial issue because the current demonstration process takes about 7 to 10 years, and thus following this path would lead to no serious cost containment for the next decade.
Here’s what ticks me off: The ObamaCare Marketplace — supported by Obama (personally), and Cutler (personally) — is a health care experiment, where proven solutions already exist (see the charts), on a captive population, without their informed consent. ObamaCare’s test subjects are captives because of the mandate; and if they consented to participate, they were not informed of alternatives to the experiment, because the administration and the Democratic nomenklatura systematically censored single payer advocacy — the obvious alternative to being experimented upon — throughout the passage of ObamaCare. It should not be necessary to say that experimenting on consumers patients without informed consent is a gross violation of medical ethics. Bogus experiment; no informed consent; captive population. Does that remind you of anything? That’s right: the Tuskegee experiments. Except, to be fair, on a much larger scale.
So how did Cutler get involved in such an intellectually and morally corrupt endeavor? I have no idea, but I would speculate TINA: In our neo-liberal regime, There Is No Alternative to a market-based solution. And for whatever reason, it does not seem to have occured to Cutler to seek to create one.[5]
And here’s the second thing that ticks me off, but this is a lot shorter and simpler: Cutler keeps calling me a “consumer,” and that gives me the creeps. I think of myself as a patient or a citizen. A commenter at PBS says this better than I can:
I get so tired of listening to people like Harvard’s David Cutler referring to healthcare patients as consumers. Like I am going out to buy a TV rather than wondering if the experts are going to be able to save my life while sick as a dog.
And more skin in the game. As if when I am in a car accident or have a heart attack or kidney stones or diabetes, a patient has any real choices except to deal with the bills assuming they survive.
So when the severe debilitating chest pain hits, I The Consumer comparison shop for the best ambulance, and while I’m on the road, I direct the driver, between spasms, to the in-network hospital, even though it’s thirty miles away, and then I comparison shop for the cheapest room, and when I’m in bed, I pop open my laptop, and comparison shop for the cheapest surgeon…. And the cheapest drugs… Because I’ve got “skin in the game”…. Even if it’s not a game…. To me… Well, Cutler puts it less vividly but more succinctly:
The trend in health care nationally is to put more and more on the patient.
What could go wrong? Consumer, my sweet Aunt Fanny. Are these people demented?
NOTES
[1] Klein’s link to the National Geographic article, by Michelle Andrews, has rotted, but the article is well attested. Here’s a useful critique of the infographic. I’m not sure why Mexico’s costs parallel the normal countries, and not the exceptional United States. Perhaps the IMSS played a mitigating role?
[2] Yet another chart showing a mid-70s inflection point at the beginning of the neo-liberal dispensation. Yes, the problem with the label on the axes exists in the original.
[3] It is true that the growth of health care spending in the United States has slowed, as would be expected, given a continued economic depression. (Dean Baker argues that although the economy has recovered, spending is still slowing, so ObamaCare must be the cause of the spending slowdown. Some recovery, if you look at labor force participation, persistently high unemployment, and lousy jobs.)
[4] ObamaCare, despite at best careless rhetoric by its advocates, is not universal and will not be even when fully implemented in 2017, causing thousands of excess deaths.
[5] David Cutler, Health Affairs, 2010. Note lack of agency:
A single-payer system was never seriously considered in the recent debate…
Acknowledgements
David Cutler was an adviser to the Obama administration during the development of the legislation discussed in this paper.
NOTE Here’s a handy chart from PNHP that summarize the differences between the ACA (ObamaCare) and single payer. Well done, Democrats!


Are these people demented?
Yes.
Of course he views us producers as consumers and the rentier class as producers.
Of course to him all values are economic.
Of course he’s a classist bourgeois in favor of class war against his many inferiors.
The minute we stop listening to virtually any member of the Military-Industrial-Academic-Complex–and the farther up the food chain, the more compromised they tend to be–is the minute we start to regain whatever freedom we had to determine our future.
Add to that, my years of experience at a certain Ivy League school impressed on me that for every wicked smart person there, there was at least one who was just wicked: smart with no heart.
Demented? Not at all–policy makers are very rational given the vision they have. What they do not talk about is the goal of the system and what politics actually is.
American political parties are, basically, power-brokerage houses. Policies are negotiated on the basis of the long-term national interest but on the basis of the power of the stake-holders. Negotiations occur and compromises are reached according to the political fire-power of each group. Good politicians manage to add on something that will benefit the public and mediocre ones will add on stuff that appears to benefit the public.
Sadly, the public and, in particular, the American left does not fully grasp this dynamic. They believe that politicians are bad or good based on the policies they advocate–but that’s not their role! Their role (with some notable exceptions) is to negotiate with those that bring the biggest guns to the table.
What is Harvard? Cutler is full of it. And sadly, Obamacare has way too many options for the non-affluent that are abusive, demented and vengeful. Have you looked at the Bronze plan? Unless you undergo major surgery, the plan pays zilch. Did we need Obamacare for that?
Probably for the first time ever, I agree with Lambert.
… and if you DO undergo major surgery, NONE of the plans, including platinum, pay much of anything for those members of your team who are out of network, which could be a great number of them.
Even before Obamacare, I’d come to understand that health insurance in the USA, at any level from the most basic “catastrophic” plan to executive-type “cadillac” plans, offer only the illusion of protection. The premiums correlated mainly with the seriousness of the health condition at which the illusion would be shattered.
I’m remembering a story in the Sunday NYT Magazine back in the summer, the focus of which was quality of life/end of life issues, that mentioned only in the briefest passing that after one member of the couple became quadraplegic, they are now paying $250,000 per year for his care ABOVE what his very-good insurance pays. And I’m remembering my father-in-law, who spent his last months in extreme suffering, because although he had the wealth to have two doctors on staff 24/7, his home health agency would not assign a second aide to him, even though two persons were needed to move him and my mother-in-law is far too frail to assist, since neither Medicare nor his supplemental insurance would cover it. His insurance dictated the care he received even though he could’ve paid for better out of pocket.
Shorter Cutler: Let’s use the government to mandate the purchase by all Americans of corporate insurance, and see if that works to lower the cost and provide exceptional service.
Shorter Lambert: WTF?!?!
Isn’t there a computer model at Harvard for this type of fantasyland type of social engineering that Cutler could focus his mightily-educated mind on instead?
Shorter lambert: You want me to be your human guinea pig? Not thanks, buster.
* * *
I just can’t emphasize enough — or rather, haven’t figured out the right language to emphasize this enough — how how unethical ObamaCare’s emplementation has been. It really and true is a medical experiment without people’s informed consent. That’s a wrong as you can get; ethically, it’s in “lampshades made from human skin” territory, for all the blandly corporate language and ideological dressing up.
People should take this very, very personally.
I agree with you 100%. But aren’t we making here a more sophisticated version of the “death panels” argument? And where does NC stand — at this point — on cooperating or not with Tea Party types on this issue?
(I’m serious, not trolling — so no whinging!)
I can’t comment on the NC position, but, regarding a particular issue such as health care, I don’t care if a person is a radical, tea party member, centrist, or what “affiliation” they may have if they agree with me on the issue…in this case, a single payer type system. I would shake their hand, say “let’s fight for this issue together”, attend meetings, etc.
truth is truth, regardless of who says it.
then again, since we’re in the post-modern world, is there any truth?
i’m so confused…
IMO really the only power we have against The Corporation in its many forms is boycotting.
So screw the ACA, pay your fine, if you really get sick a r/t plane ticket to any number of more advanced countries plus out-of-pocket will still probably save you money, and even if it doesn’t millions opting out may be enough to starve this beast and help bring about single-payer or medicare for all.
No pain, no gain.
Verily, verily, Lambert, your outrage is as good as it gets. You’ve taken a literary whip to the money-changers in the temple of democracy. Pharisees and high priests like Odious-O and Cutler, both alumni of Harvard, are little more than harlots for death-panel insurance rackets.
Based on what standard of ethics, Lambert? Cutler and the Obama operatives deal with reality. They deal with real power and they negotiate with people who are armed to the teeth, as they see it. They believe they got the best deal they were going to get–and you and I agree that it may be worse than what was before but I believe they think it was the best they could get.
Are you going to tell the industry that it can’t gouge the American public anymore? You think you can shame them into compliance? I submit that Obama, even if he wanted to, is powerless to force major power-players to submit to a sense of common purpose. The last President who was able to do that was killed for it (and other sins) 50 years ago yesterday.
Well said. I don’t like many things Obama is doing when I think he has a choice, for example his choice of Treasury Secretary and other appointments. But for the ACA I think he was thinking out of the box and as you say had little choice. I don’t think that Big Pharma or Big Insurance had any idea of how it would play out and indeed no one has a crystal ball. One thing is certain, change. Is it the change we hoped it would be? Time will tell but forcing the insured to look at why their premiums are high is in my opinion a very good idea. It forces people to get involved and find out why. Currently questionable treatments, scans and drugs have been able to maim and kill for far too long while industry covers it up and goes on marketing its products. And many people are so enamored with doctors and medicine in general it is hard to reach them. Now we’ll have millions of Americans wanting change and in my mind, is a good outcome. Granted it doesn’t solve the problems but it is forcing the conversation to change and exposing the corruption in medicine.
The mandate is to make it possible for people with pre-existing conditions to get insurance. It’s not primarily to reduce costs, although it does some by eliminating the waste of underwriting, and we’ve seen that with the exchange plans coming in under expectations.
The real cost savings from Obamacare come through a lot of complex regulations which basically boil down to “they’re not going to pay for things that actually make the patient worse”. Those are actually working considerably better than expected, and even after adjusting for the poor economy, we’ve seen the lowest increases in per capita cost that we’ve seen for decades – while outcomes have actually been improving.
Do you have a source for those claims?
BTW, I don’t know what kind of “economist” can’t get his head around the fact that a mandate is not the only way to help those with pre-existing conditions. For some people, being poor is a “pre-existing condition,” but they get welfare right enough — they don’t have to be mandated into some kind of Rube Goldberg “system.”
What we’re doing now, in order to provide medical welfare to those who might need it, is to have everyone give a form of “welfare” (via the mandate) to those poor wittle insurance companies. Clearly this is another aspect of the TINA problem.
Sure, here’s the drop in readmission rates: http://www.fiercehealthcare.com/story/cms-readmission-rates-drop-threat-penalties/2013-03-01
A mandate isn’t the only way, but it works far better than direct subsidies to pre-existing conditions (which create monstrous fraud opportunities; overwriting high for subsidized patients is pure profit). True socialized medicine is much more efficient, but that wasn’t going to happen.
Not everyone. Just the previously uninsured and the formerly insured who purchased in the individual market. Had the costs been born universally, the Obamacare plans would have been less onerously expensive and cruddy.
They are hit the hardest, but actually everyone’s premiums are going up and noone knows how much longer employers will keep their plans (plus anyone’s who plan is deemed “Cadillac” loses, some unions who had truly good humane healthcare plans lose etc.).
But … but … premiums were going up before Obamacare. Yes and a healthcare “reform” that doesn’t deal with rising costs is dubious.
Just the competition part of this travesty of a mandate causes inflated prices for “consumers”.
If healthy people paying premiums to cover sick people is the goal, and the reason for the mandate, the only way to get the best value is to have all of the healthy people and sick people – everyone – in one plan.
If bargaining power (cost control) is the goal, the largest plan has the most bargaining power so the maximum bargaining power is with everyone in one plan.
These are the “market” arguments I keep hearing over and over again from the so called experts. They fail to point out that these exact arguments point toward some single payer system as being a better value than competition, since competition will separate people into different groups and having multiple groups reduces bargaining power.
I’m probably preaching to the choir here, but I have yet to hear anyone point this out to the [shills] experts in the media or even on call-in shows.
there was an article here recently that I think was done by the NYT, in which the pharma-tech-lobbyist-venture capital guy who was starting up a new business in the medical world said basically “they promised us we could all get rich, as long as we controlled the costs of the doctors & hospitals”.
so, his understanding, which it was suggested he got from the political classes he swam in, was that they would use the power of one group of vested interests against the other.
I don’t deny what you’re saying at all. it seems dead-on correct. but IF the ‘real’ aim was to drive down those hoity-toity doctors and hospital administrators (whom I guess it can be perceived as having a form of monopoly on the actual ‘health care’ provided, because they are the ones really providing it) then I just wonder why this group is so powerful that they couldn’t see what was coming and lobby against it.
the whole thing is strange. then again, one can’t rule out that what the politicians do is tell everyone what they want to hear, and that their provided solution is the golden ticket to achieving it.
Well, I’d rather address this to a good economist rather than to a merely fair one, but pray tell dear dismal scientist what’s so bad about Medicare for all or single payer? How is keeping a for-profit system in place the best option?
Despite being only a fair economist, don’t waste my time with the specious capitalist argument about the sacrosanct profit motive (see charts above). How does having a middle-man between me and my cheese make things better for anyone but the middle man? I’m all ears.
You’re not serious, are you? You honestly think having a government monopoly healthcare system DELETES the middle man?
If you’re truly full on against the dreaded profit motive, I’ll foot the bill for a one way plane ticket to Venezuela….they’re doing it your way so you’ll feel right at home.
Or a one way plane ticket to Canada. NO!!!!!! Not Canada!
Those reductions have little to do with Obamacare. The industry was reaching the laws of diminishing returns. Parts of the industry was able to make pragmatic reforms on its own which, in my view, would have continued without Obamacare.
The point here is that we still reward larceny in this system. The industry is very wasteful and full of fraud and waste. The industry came to finally believe that it was time for stability and agreed to a limit to greed in exchange for a stable but still outrageous revenue flow.
We Figured this Out at the University of Magonia Already
This is just plain supply and demand.
Since life expectancy is going down, you’d expect health care costs to go up! This is only natural, since life expectancy is part of the consumer utility function and utility maximization by rational economic agents is the way things work.
People want life expectancy to go up, so they pay more! It’s just like ordering that 3rd beer at the bar on a Friday night.
When the supply/demand equation reaches equilibrium, life expectancy will be stable and costs will be stable.
I always liked the idea of consumer shopping and negotiating prices with the surgeon/hospital while under anesthetic. Sound like a challenge. Maybe there is a Harvard MBA course on that?
I did start carrying a band-aid in my wallet thinking I can save $40 that way.
Because healthcare is so fun, it’s like chocolate cake, I have to stop myself before consuming more and more of it. It’s like big gulps, they are reducing our consumption for our own benefit, because otherwise the temptation is too much to resist!
Well no I can think of about 1000 things in a consumer economy I’d rather spend my money on than healthcare, about a 1000 places I’d rather hang out than doctors offices and hospitals. While it’s true people in this country live a pretty unhealthy lifestyle this isn’t so easily reversed by the time one is seeking medical care (yea some heart issues can be, but diabetes for instance is usually only managed). And yes things are OVERPRESCIBED which leads to excessive money spent on healthcare! But if they really wanted to address that in addition to cost penalties for us wouldn’t they ban pharma advertising (carrot and stick you know). But they didnt’. It’s almost like they aren’t serious about reducing medical costs.
Almost!
I love the way you put this. like we WANT to be there, praying for a solution, being fobbed off with drugs, and just hoping that whatever they are going to do to us works.
we don’t like this model of medical ‘care’ any more than the ones who think we use too much of it do. this whole thing should be re-oriented around prevention.
why don’t they do that? because then, just like the educational debate and inequities and results there, our society might have to truly address the fundamental underlying cause of all of this–poverty, and a system which makes money off of keeping people poor, ill fed, and sickly needing drugs.
we are like cows being milked here, and we KNOW it!
Tiring of people like Harvard’s David Cutler calling us “consumers” …
Paul Krugman’s question:
“How did it become normal, or for that matter even acceptable, to refer to medical patients as ‘consumers’? The relationship between patient and doctor used to be considered something special, almost sacred. Now politicians and supposed reformers talk about the act of receiving care as if it were no different from a commercial transaction, like buying a car — and their only complaint is that it isn’t commercial enough. What has gone wrong with us?”
http://www.nytimes.com/2011/04/22/opinion/22krugman.html?_r=0
Another of my pet peeves is the patronizing political use of “folks.”
Obama, in particular, calls us “folks” all the time. It drives me absolutely crazy.
Susan Jacoby, The Age of American Unreason, writes:
“Substitute folks for people, farmer, old men, widows, and the relationship between the abandonment of dignified public speech and the degradation of the political process becomes clear. To call for resolution and a spirit of patriotism and sacrifice is to call upon people to rise above their everyday selves and to behave as true citizens. To keep telling Americans that they are just folks to expect nothing special – a ratification and exaltation of the quotidian that is one of the distinguishing marks of anti-intellectualism in any era.”
Yes….emphatic agreement on “consumers” and “folks.” The folks thing is like something out of Vonnegut. There are a handful of us holding out, but you hear it everywhere.
Besides lowering expectations…there is the other side, making international criminals just regular guys. “The folks at McDonalds,” or Chase, or the Pentagon.
Chomsky had something on this a long time ago too….
It’s not comparable, But Lambert S. is pretty discouraging where language is concerned. Cutler “ticks me off.” Is that really the phrase for discussing health care in the US?
Even worse, this from the column–
“Does that remind you of anything? That’s right: the Tuskegee experiments. Except, to be fair, on a much larger scale.”
That is bizarre. First the comparison itself. The Republicans call it slavery…Strether say it is like injecting prisoners with people syphilis? (Was there no 3rd Reich image available??). But also, when he writes,
“that’s right…” in answer to his own rhetorical question. I would love to know how many readers thought of Tuskegee independently as they read. My guess is zero.
Also on the language front. Krugman’s comments on “consumer” were excellent. But he is a pioneer in the new casual, jokey writing style.
Thanks for your comment.
I could be wrong about this…lord knows what they actually did in the Tuskegee STudy was evil enough, but to my knowledge they did not inject people with syphilis.
the found people who already had it, didn’t inform them that syphilis was what they had (saying instead it was a vague ‘blood disorder’), told them they WERE being treated for it which is why they had to keep coming back into see the doctors/researchers, tried to dissuade them from getting care for it elsewhere (“you tell them doctors that we’re treating you for this, ok?”), allowed their wives and children to contract it, and all done mostly while we HAD already developed a cure for it. this was done to supposedly study the long term effects of a disease which had been plaguing humanity for how many hundreds of years? in other words, we already KNEW what untreated syphilis could do to you BEFORE WE HAD A TREATMENT!
which somehow shows that, without taking direct action against someone you can be truly evil. and I don’t care how ‘trite’ Russell Brand and his relativist ilk believe that term to be (I do understand his greater point re: externalization and rejection of behaviors that we’re all capable of, but a duck is a duck, dude!).
is this rather like the positive and negative rights discussion? positive and negative evil.
If getting “evil” people out of positions actually worked on a long-term basis, wouldn’t it have by now? The concepts of “evil” and “good” are designed to replace understanding with emotion, systems analysis with cheap easy scapegoating, and self-awareness with blind jingoism.
In other words, the very same thinking that got us into this mess, and Einstein had something to say about that.
Please stop promoting the fundamental attribution error. It’s Romantic cargo-cult thinking with zero predictive utility.
I said nothing about ‘evil’ individuals. the rest of your rant is totally irrelevant to my point.
there is evil behavior. to deny the existence of evil means that we have nothing that is beyond the bounds of what most would consider ‘moral’ behavior. to learn that every individual is capable of it, and that we tend to call whatever someone ELSE does that we don’t agree with, but would manage to justify that same behavior if we somehow ‘needed’ to do it, is just another level of nuance that is necessary. to say there is nothing evil means we have no basis to compare anything, and therefore Anything might be justifiable under the right circumstances.
are there ANY circumstances under which you could see the Tuskegee STudy (without changing the details of the story–like “we never found the cure and so could not do anything about it, but we COULD study it!”) justifiable? no…it was evil, pure and simple. whether the individuals involved were evil or not, I couldn’t tell you.
but I have met evil individuals. and they were honestly EVIL. I don’t think smashing your wife’s face in with a pistol so hard that she was breathing through the flesh in her cheek is really justifiable, at least…not unless she was trying to kill him or something (which she wasn’t. she was sleeping). I don’t think that this, in combination with all of that particular person’s other behaviors, was ever justifiable. I think this person was what we would term “evil”, which could merely mean that they had a personality disorder which was not ever going to be amenable to treatment.
please don’t fundamentally attribute to me what i’m not really sayin’.
It is very important, at some point, to define terms because we live at a time of very broad disagreement on what is “good” and “evil.” In society we need to have some common agreement on these terms because political and economic issues depend on morality which, in turn, depends on some metaphysical/philosophical framework.
Changing the reference from ‘Citizen’ to ‘Consumer’ was a deliberate strategy by Edward Bernays who was the creator of modern Public Relations and nephew of Sigmond Freud…
‘Citizen’ implies an activist responsibility
‘Consumer’ is a degradation indicating our primary occupation is consumption (to satisfy profits).
Noam Chomsky’s book ‘Manufacturing Consent’ brilliantly picks apart how linguistic framework in the media and elsewhere pervasively manipulates the population.
Post Script….4 minutes after posting, I read the following in the Columbia Review of Journalism—
“Not only that, but your political opponents—the folks who can’t afford to buy your ads—will get ignored at best.”
It’s an epidemic.
Thanks a million for the quote. I’m very happy to find that other people hate the word “folks” as much as I do.
This is link- or at least cite worthy (despite being from 2008): the Susan Jacoby article from which that quote is drawn.
Where were you with this when fromMexico was scolding me for being critical of my compatriots lack of interest in current affairs or the political process? He accused me of stereotyping and being haughty and unkind. I don’t know if I was or not, but Ms. Jacoby puts it in much less assailable terms.
The rhetoric of neo-liberalism is brutal. Why are employees ‘associates?’ Why are patients ‘consumers?’
Because we’re not responsible for anything we do, no matter what, but you are, and also, for the record, fuck you.
Sounds more like Cutler is wickedly twisted. Perhaps Harvard isn’t necessarily a beacon of intellectual prowess, but more an incubator of moral turpitude.
Gee, ya think?
Obamacare can be understood as outlawing the exit option. Allowing exit is a way of thinking Cutler will not broach because his social status, income power depend upon pretending citizens are “customers”. Surely Lambert’s introduction of Cutler “he’s from Harvard, and he’s wicked smart,” is facetious. Cutler’s just wicked, as are Rogoff and Reinhart, also at Harvard.
Harvard threw itself almost 100% into the endowment maximization business back in the 80s, and they haven’t been worth a crap since. The Harvard name used to mean something. Now it’s just being tossed around to see how much money they can suck out of it. What a shame.
$2.5 million was the going minimum a decade ago to get your kid into Harvard. Anyone know how much the price has risen?
An interesting Counterpunch piece that harmonizes nicely with Lambert’s expose of Harvard’s best and brightest:
An Orgy of Thieves
“Back in the mists of antiquity, you had communists and socialists and populists who’d read Marx, and who had a pretty fair notion of what the rich were up to. Even Democrats had a grasp of the true situation. Then came the witchhunts and the buyouts, hand in hand. Result, a Goldman Sachs trader could come to maturity without ever once hearing an admonitory word about it being wrong to lie, cheat and steal, sell out your co-workers, defraud your customers.
The finest schools in America educated a criminal elite that stole the store in less than a decade. Was it all the fault of Ayn Rand, of the Chicago School, of Hollywood, of God’s demise?”
http://www.counterpunch.org/2013/11/22/an-orgy-of-thieves/
I think the structural mechanism goes back to Watergate. First, the GOP was always the GOP with a few isolated spots such as Massachusetts’ GOP, and so they are irrelevant.
After Watergate, there was a major move by the Democrats to avoid the anti-Washington fervor by recruiting non-Democrats to be candidates instead opting for candidates the GOP wouldn’t attack and who could self-fund. Throw in a few celebrity candidates (Al Gore Jr. and Evan Bayh), and you get a decrepit party full of people who possess no moral center. In essence, they were recruited because they weren’t offensive to anyone. Since no one recognizes a profit in their own land, good people offend, and the Democratic Party is dominated by amoral people. The nomination process is so difficult its tough to retake the party from these people without them giving up.
Since they are usually friendly, people at the lower levels give them the benefit of the doubt, and admittedly, I think there is a sense being good and moral is easy and applied to most people.
I do think there is a structural problem in the Democratic Party, and in a sense Liz Warren is a good example of this. She’s pro-imperialism which is not a polled position of the Democratic voter, but she’s becoming loved because she is so much better than the average Democratic elite despite holding radical positions shared by 70% of the population such as being pro-choice, pro-Social Security, and advocating changes to credit cards which would have been great in the 1980’s. Warren is our great white hope. This is terrifying.
A common fallacy in your assumptions is that longevity correlates with the quality of health care which is also the only predictor of longevity. The fact is longevity (and infant mortality for that matter) have more to do with lifestyle behaviors (diet, exercise, drug use, violence, accidents, like autos, etc.) than with the quality and volume of health care. The quality of health care (more properly called sick care) should be reflected by how well and long people survive after an actual medical condition exists.
The US spends enormous sums on cancer therapies that offer pitifully little in terms life extension. We also spends lots of money on treatments for chronic diseases that create side effects that must be treated and keep the patients coming back for more health care. In the long run we’re now preventing disease, but merely delaying it until the patient is older and likely to require more health care.
I noticed that too (and to be fair Lambert included a little qualifying aside), lots of other factors play into that life expectancy number.
I also often wonder in these country to country comparisons, if it’s misleading to draw conclusions about the US because of our high GINI coefficient (or without the jargon– wealth disparity.) The “Two Americas” as John Edwards called it, confuses the issue when comparing to more homogenous developed Euro countries. Let’s break it down and see “rich America” and “poor America” separately compared to Euro land. The health care experiences of the 51%, and especially the 20%, are much different from the 49% (although maybe with Medicare, and most health dollars spent at end of life, maybe it’s not that big an issue…)
And also to your point on the value of the care itself MGK, Cutler himself says in the interview that Canada has far, far fewer open heart surgeries after heart attacks than the US, but equal health outcomes for those patients!! Clearly, the miracle of modern medicine, at least in that case, is exposed as a sham of wishful thinking and science fetishism (and profit-seeking.) In the 19th century, a road diverged in the woods between allopathic medicine and homeopathic medicine and we, well, we took the Rockefeller controlled, centralized and monopolized allopathic road of radical surgery and petrochemical pharmaceuticals that treat symptoms not causes, and that has made all the difference.
Well, I won’t knock it entirely– I subscribe to Paul Jaminet’s (perfecthealthdiet.com) view that modern medicine is very useful for lab tests (identifying pathogens, etc.), and intensive antibiotics when/if homeopathic techniques are inadequate; but then, homeopathic techniques of diet and lifestyle are best to heal and nurture the body- *try* to avoid getting put on a regimen of pharmaceuticals if possible…!
No, heart bypasses *do* make a big difference for some patients. It’s just that that’s a smallish subset of all heart attack patients – those with disease affecting their left ventricular blood supply, roughly. *Those* patients get bypasses both here and in Canada, so Canadians do get the benefits of bypass surgery. The additional patients, who get it in the US, get only temporary symptomatic relief on average.
The problem is not that modern medical procedures don’t help – they usually do (although not always). They problem is that the person deciding whether to use them (usually the doctor doing the surgery, or one of their associates) gets paid a bonus for their use. So they’re grossly overused – sometimes even to the point where they’re bad for the patient. That includes bypass surgery, with “pump head” (brain damage from circulatory changes during bypass), direct surgical complication, and limited mobility from stripping the leg veins.
‘We spend lots of money on treatments for chronic diseases that create side effects that must be treated and keep the patients coming back for more health care.’
Escape Fire, a documentary about health reform, points out that U.S. ag policy subsidizes wheat, sugar and corn (and thus, HFCS-laden junk food), while fruits and vegetables cost market price.
http://www.escapefiremovie.com/
With one of the most obese populations on earth, of course the U.S. incurs ‘global outlier’ costs for symptomatic treatment of the resulting chronic diseases (such as diabetes).
‘Skin in the game’ used to work in the U.S. (roughly until the Medicare/Medicaid monster was created in 1965), and still does work in other places. But in the cartelized U.S. health system (hospital cartel, Big Pharma cartel, physicians’ guild, malpractice attorneys’ guild, etc.) with its unaccountable price-discriminatory, cost-plus model, market discipline can’t function.
Under our corrupt Depublicrat regime, single-payer would protect and entrench these cartels, just as surely as Obamacare does. The cost to ‘consumers’ might even exceed my exorbitant school taxes (thousands a year to another unaccountable single-payer service provider).
Remember: there is no such thing as ‘reform’ under an entrenched duopoly. Smash the state!
Or get a state that will absolutely smash pharma, the hospital cartels etc. etc.. Because I see no way forward in any system that doesn’t completely salt the earth for them and the existing insurance companies. Or maybe it will just happen in all but emergency cases anyway, as everyone goes to another country for medical care, since the U.S. system is hopeless.
By the way is going to other countries for healthcare being a “smart price sensitive consumer fully utilizing the marketplace?”
If that ever passes a certain point, I’m sure they’ll try to illegalize it to the extent that they can.
Before that point, if your money is already being extracted by the U.S. government and handed over to the medical-industrial complex, then it’s a win for them if you actually go elsewhere for your real medical services.
SES is a better predictor of longevity than ‘lifestyle behaviors”.
SES is merely a correlate for lifestyle behaviors. I recall a study that estimated at least 50% of racial longevity disparity can be accounted for by controlling for education, which is likely to impact both SES and lifestyle behaviors.
No, it is not. There was a whole book written about it. Actually, it was about inequality and poor health outcomes and it was based on this study which did about as well as you could controlling for variables.
http://en.wikipedia.org/wiki/Whitehall_Studies
With roughly 40% of the variation accounted for by lifestyles behaviors, I say that it is still a pretty good correlate. At the same time, you’ll notice that education was not controlled for in their analysis. I suspect that was because education was highly correlated with their civil service position and thus directly contributed to their status.
Or SES has an impact on educational level more likely.
what does that imply to you? that people with lower SES should be blamed for their lifestyle causing their health problems?
isn’t this much like the education/IQ link?
how much is an individual supposed to be responsible for, when all they can afford is canned greyish green beans and fried chicken? we’re talking poor people culture here. you think they LIKE living that way? it’s essential, at that price point.
i’ve eat so damned many grey looking canned vegetables in my lifetime, and poor cuts of meat (when we had them, and i wasn’t a vegmuhtarian) and AgroBiz concoctions (hey, Manwich is cheap!) when i would’ve rather had fresh fruits and vegis and such. but that crap costs quite a bit more, needs to be fresh and expires VERY quickly. when you don’t have the time to shop except in bits and snatches, you will rely on boxed/canned food.
one might make the argument that poor people don’t ‘know any better’, and that might be true after a few generations of this and not being trained how to cook properly (i speak from experience here), but there are just way too many factors having to do with money & time & resources available here.
so, SES, or lifestyle, or both are related, or what? why does this make much of a difference in the end? to an actual poor person, the only way they’re going to be able to make the proper lifestyle choices is if they have the money, time and skills/tools to do so.
my aunt goes running in the ghetto every morning to this day. she is a crazy white lady, and she’s taking her life in her hands every time she does this. plus, she’s lucky enough to have a job that doesn’t start until later in the afternoon. for peope who have to get their kids off to school in the morning (with or without breakfast), and get their asses to work on public transit, and do manual or menial (often both at once) work every day, and come home and try to get the kids fed and all, i don’t fault them for not wanting to do 1hr of pilates workout. do you?
sheeze…
It’s not about blame, but about recognizing the difference between correlation and causation. The potential pitfall is that you focus efforts merely on a correlate and when you don’t see the expected change you come up with more convoluted reasons and just do more of the same. There’s been high and low SESs for centuries and during most of that time no one had much health care to speak of, but in the last 50 years have we seen an explosion in the number of people with obesity and diabetes. It’s not class distinction that causing the problem.
well, thank you for clarifying that this is about determining true causation, and not merely saying “individuals cause their own problems”, although I would remind you that this is exactly how what you are discussing gets simplified in the larger discourse.
could it be subsidized food, and which food is subsidized itself? subsidized food is cheaper, they put it into everything (especially the boxed food, because it’s cheap), and that may be what is causing it?
you’ve also got activity levels, and everything. there are a massive number of intersections on this. and yet, every time someone identifies one element, they tend to latch onto that and ‘blame’ the person for ‘willingly’ allowing that to effect them, without recognition of the interplay of factors. hence, my worry.
Indeed, cancer costs a lot. Mine so far is up in the $300 thousand range, and I’ve got what is generally considered terminal cancer. What a waste of money, huh?
Ooops, just got my latest PET scan back. ($3000 for that test!) Says there’s been significant shrinkage. I might live after all.
OK, maybe I’m shot in the dark. Maybe most people with my cancer still do die. But ALL OF THEM DID twenty years ago. And that’s how medicine grows and gets better. One or two successes this year, ten or twenty a few years down, and after a time, it’s considered curable.
Which will be great in the future when others get it. Like maybe you. Or someone you love. Will you still think then about the “enormous sums on cancer therapies that offer pitifully little”?
Thanks for making this point I was about to myself, and probably much better than I could have. It is indeed sick care we’re talking about, just one more of the Orwelliansims that saturate our discourse.
I’m not preaching here as I too have gotten too sedintary, but exercise, good food and water, and enough sleep will prevent most of the chronic “diseases” we suffer from (again, I’m far from perfect on any but the middle one). Spend a little time in Asia and the mostly slim, graceful LBM men and women really make most of the visiting tourists look like grotesque caricatures of human beings; that’s what our “wealth” has done to us.
When you consider the theory that Jesus was an Essene his words on poverty take on a whole new meaning.
I believe that is partially right but beside the point. Actually, it isn’t so much “lifestyle” issues but stress that determines health, i.e, cortisol. We could scrap our whole system today and dramatically improve longevity and health if we got really, really, mellllllow and partied more and worked less. Of course, I’m not completely serious–public health, vaccinations, good sewers, environmental regs, cleanliness (but not too much) and a few other things are requirements for a healthy society.
Kudos Lambert!
I was initially surprised by your reverence towards the Harvard credential but your irreverence eventually shone through and pierced the veil of that imaginary delineator of human value. Some Harvard employees are smart. Many are. However, one goal of my career choice was to find smart people to converse with and my experience in academia has been mixed with only a low (and sometimes seemingly negative) correlation between institutional status and individual insight-intelligence. (aside from the fact that you are smart, i.e., quick in comprehending, analyzing and critiquing ideas) Additionally, my egalitarian beliefs compel me to respect and seek wisdom and insight from any person. Insights and pivotal ideas arise everywhere; and individual insight and accuracy is usually inconsistent. I feel compelled to be irreverent of elitism because equal respect matches my egalitarian beliefs. You can school an expert just like any of us can – equal voice is almost a motto, precept, and part of the identity of the blogosphere. Truth and reason trump status.
Correction: “…equal voice is almost a motto, precept, and part of the identity of blogs like NC
the blogosphere.”The slope of the US line in the first graph is so off-the-charts, it could be inferred that the US is actually spending all that money to KILL people.
Boston, where I live, is the epicenter of the health care industrial complex. Norvatis is erecting a huge building in Cambridge, and “health care” is all around us. Building a community one presecription and illness at a time should be the motto. The fear must run deep that we will awaken from our slumber and wring out all of the waste, sucking profits from the health care vendors.
You are unlikely to find many “academics” around here advocating single payer when their pay, and city, so depend on keeping the status quo. As they say, never trust a person to weigh in on an issue when their paycheck (or lifestyle) is dependent on it turning out a certain way.
The way I see things, physicians at the bedside are getting squeezed, while the ones in the back office are living high on the hog. I see it and hear about it every day, and it’s only getting worse. This is because healthcare providers have unwisely decided to increase salaries for executive physicians and reduce salaries for clinical physicians.
As to who or what deserves most of the blame for this gross as well as growing misallocation of the healthcare dollars, which is bound to harm patients in the end ( not just their health, but their pocketbooks as well), I would pin it on the for-profit insurance industry, and at the heart of this industry is the wobbly, unwieldy, bureaucratic Rube Goldberg machine known as ObamaCare. ObamaCare is so unbelievably complex and convoluted in the way it rewards and penalizes hospitals, hospitals have hired wiz kids in administration with very crooked minds, which gives them the necessary skills to traverse themselves through the rat maze of red tape. The better they can do this, the bigger the bonuses they get; and believe me, none of this bonus money trickles down to those of us laboring away in the clinical setting.
The best we can hope for is for ObamaCare to fall on its own sword.
Woulad like to hear more comments on costs of adminstration. Where is Susan the Other?
What a joke. “Skin in the game.” What do you think the medical industrial complex would do if everyone was to say “yes, I think I’ll opt for conservative medical management of my partially blocked arteries”.
Here’s my thoughts: they market their surgical/interventional radiology services harder, or they make conservative medical treatment more expensive, or failing that they find something new to sell us.
Celebrating the slowdown in health care spending!
Jason Furman, chairman of White House Council of Economic Advisers, is trumpeting that “health care spending and prices are growing at their slowest rates in decades; it appears that something has changed for the better.”
http://www.whitehouse.gov/blog/2013/11/20/new-report-from-council-economic-advisers-recent
What could that something possibly be?
Why of course, “the available evidence suggests that the Affordable Care Act is contributing to these trends, and, moreover, is helping to improve quality of care for patients.”
“Or so it seems that is what they want us to believe,” says Don McCanne MD @ PNHP:
“Furman tends to minimize two important factors as he touts the great benefits of the Affordable Care Act:
• the weak economy that persists since the Great Recession
• the expansion of health insurance products that place more of the burden of paying for health care on patients themselves
“Prices and volume determine the level of spending. The continuing weakness in the economy has created a reluctance to increase prices, and the cost sharing barriers such as high-deductibles have decreased the volume of services accessed. Spending slows.
“So should we nevertheless be celebrating the slowdown in health care spending? Let’s look at the score sheet:
Protracted weak economy – No celebration
Impaired access to care through cost barriers – No celebration
Ineffective policies of the Affordable Care Act – No celebration
Good grief!”
http://pnhp.org/blog/2013/11/21/why-we-shouldnt-be-celebrating-the-slowdown-in-health-care-spending/
We should see in coming years declines in various health status indices and in broad public health factors summed up by the concept of social determinants of health. For instance, there are several counties in the US where average life expectancy has begun to fall.
Yes. I believe that (exactly as with permanently high unemployment) that is the unstated elite policy goal.
Shorter: That’s not a bug. It’s a feature.
Maybe the reason for the slowdown in price increases (they are still increasing, mind you) is that there’s only so much a society can spend on healthcare before other competing needs rise enough in priority to act as a brake. What I’d be interested in seeing is whether it is simply total spending that is slowing, or whether total spending was slowing because prices for individual procedures were slowing. If it’s the former, it probably means that fewer and fewer services will be offered for higher and higher prices, which is to say the ultimate in rationing is beginning: If you are rich, see your doctor. If you are poor, see your priest. All others, go to the tail end of the shortest line with your latest tax return.
Another excellent comment from you DK. This whole charade is like congratulating the worker you just fired for lowering the amount of money he spends on food as a good thing.
Healthcare costs are rising as a percentage of GNP. Just maybe, to paraphrase Ben Franklin, Americans are willing to pay up in order to be and stay healthy, wealthy, and wise. Just maybe. And just maybe we will cut back on buying other stupid things in order to achieve those blessings. Stupid things. …
As an environmentalist, I fully support American-style corporate health-care, and so should you.
We all know about the ridiculous quantities of resources the American lifestyle demands. By encouraging policies (like single-payer) that extend lifespans, you are encouraging the more rapid depletion of our precious natural resources and our ecosystems, upon which all life depends.
Consider how many more cattle would need to be raised in their feces-filled feedlots, how many more trees would need to be cut down for TP, how many more barrels of oil would need to be pumped for how many more cars, if we all lived five years longer.
And if our health-care system were cheaper, then we’d just have more to spend on resource-intensive manufactured goods. Take all this together and it’s clear as day: Single-payer would be the single greatest environmental calamity since the invention of the internal combustion engine.
Let’s face it: the only way to save the planet (in a manner fit for our continued habitation) is to lower the population and overall life expectancy of our species. I don’t see how any consistent environmentalist can advocate for better health-care (ditto for decreasing wealth inequality or gun-control).
As a consistent environmentalist, I support all of the following:
1) High-cost, poor-outcome, corporate health-care
2) Funneling as much wealth as possible to as small a number of people as possible
3) Arming every man, woman and child (especially the children) with assault weapons
4) Chain smoking
Do the environment and every other species on the planet a favor: die quick.
No doubt you will lead us with your fine example.
Aye, there’s the rub…
so, the good ol’ C of E is still around?
good to know.
That’s the ticket!!!
Interesting though is that, not to rain on your parade, that people who are happy, fulfilled and mellow don’t need to use so many resources to fill the emptiness. But funny and witty stuff!
Wait a minute. I was taking this guy Cutler seriously when you said that he was “wicked smart”. But then later on I realized that he was just an economist. Hell, might as well put a “wicked smart” astrologist here talking about this stuff, since economists and astrologists have exactly the same amount of authority when talking anything.
If you’re from Somerville (the compost heap in the back of Harvard Yard), you pronounce that “wicked smaht”….
When the severe debilitating chest pain hits, no need to pop open the laptop, there’s an app for that!
No kidding, received in my inbox this morning:
“As a UnitedHealthcare member, you can preview medical procedures, compare treatment options, estimate costs and quality ratings before receiving treatment. You’ll be more prepared to make a more informed choice.
And, since costs can vary widely based on the provider, facility and treatment you choose, as a UnitedHealthcare member, you can stay in charge and make informed decisions for your health and your pocketbook.
Make your next smart decision. Learn more today at myuhc.com®.
Then click on the Estimate Health Care Costs button.
Use the new award-winning app, UnitedHealthcare Health4Me™ to access myHealthcare Cost Estimator on mobile devices.
All UnitedHealthcare members can access a cost estimator online tool at myuhc.com. Depending on your specific benefit plan and the ZIP code that is entered, either the myHealthcare Cost Estimator or the Treatment Cost Estimator will be available. A mobile version of myHealthcare Cost Estimator is available in the Health4Me mobile app, and additional ZIP codes and procedures will be added soon.”
Laughter aside, not all healthcare is life and death. My husband is due for a colonoscopy next year, and I plan to use the app to cost compare. More price transparency in the healthcare field would be a welcome change for me, as an enrollee in a high deductible plan.
“If you’ve got a hammer…”
Except that app wont’t tell you how to avoid the facilities that don’t clean their instruments well. 15% of the time, the devices haven’t been cleaned properly.
We are also the only advance economy that recommends colonoscopies for everybody. Other countries recommend them only for people who are at risk.
See this:
http://www.protectpatientsblog.com/2012/02/testing_for_colon_cancer_offer_1.html
http://www.protectpatientsblog.com/2013/01/doctor_who_performs_colonoscop_1.html
http://www.protectpatientsblog.com/2012/05/virtual_colonoscopygood_result_1.html
http://www.protectpatientsblog.com/2008/12/new_study_reveals_surprisingly.html
You strike at one of the chief myths propagated by the accepted mythology–that we have a HC system of quality care it’s just that people many can’t afford it. The malaise in the system is very, very deep and includes how doctors and insurance companies approach healing.
As many recent studies have shown, stress is an important source of many diseases since too much cortisol in the system is toxic. Also, many promising healing modalities are ignored or repressed because of the low-probability of profit and so on and so on.
You’ll never get price transperancy until you get rid of the monopoly protections the Medical Industrial Complex enjoy under the Sherman and Clayton Acts. With those protections, they are free to price and cost shift and arbitrage to their heart’s content.
6 years ago I was given the colonoscopy speech by my doctor, a man, since retired, I highly respect. I read a lot of alternative medicine literature, told him since I’m not a high risk I’ll pass. I did, however, stop at the desk at the hospital where they schedule the procedure. Asked the gal at the desk what one will cost me…since I had, and have, a high deductible policy and Health Savings Account I pay the bill….she looked at me like I had just sprouted a third eye. Long story short, anywhere from $3, 000 to $13, 000.
You neglected to mention “transparency” the latest buzz word of the let’s shop around for health care crowd. They want all the charges clearly posted so the the informed consumer can make the best deal on their knee replacement, including parts and labor. I think that was the main focus of the AMA report that came out yesterday on reducing healthcare costs. We don’t need the government messing about and riding herd on healthcare providers since we have have the world’s smartest consumers who just need information to get the cheapest deals.
This was the ultra conservative approach many years ago and has now morphed into the status quo institutionalized by the ACA.
It is clearly insane for all the reasons you cite above.
Demented? No. Willfully blindly evil? Yes.
And you are damn right Yves about the consumer language. It’s attempting to rebrand people, much like the dropping of Obamacare for ACA language, or the introduction of red state v. blue state, which was supposed to rotate each year but was used to separate D’s from the stigma of communism, to global warming v. “climate change”.
All are rebrandings to allow manipulation of the individual citizen’s thought structure.
A Citizen has rights; Consumers are cattle to be farmed.
So I have these sizable mysterious lumps in my neck. My GP says I need to buy insurance and see an expensive specialist just to get a diagnosis. But if I spend a few k a year on insurance (which I cannot afford, until my mortgage is paid off) it won’t cover the first 6k plus of a specialist. So with O or without Obamney not care… I have these sizable mysterious lumps in my neck.
Dawg forbid, if this is cancer, would this Harvard economist and the feckless journalists at the News Hour be willing to look me and countless millions of others (with or without insurance) straight in the eye and stand by these kinds of interviews that tell me i just need to be a better consumer! Interviews which will be looked back upon with the same dismay as students of history today look back upon the dark ages?
Whatever the definition of Insurance is… Several plus thousand dollars premium with massive deductibles, and if beyond deductible limits only a 60 percent off coupon, I mean insurance, kicks in, only assures access to care remains as far away as it ever was.
My contempt for the NPR/PBS organizations continues to find new lows.
this is where ‘shopping around’ should come it. ask your doc. for referrals and state clearly that you will be paying cash. ask him/her whether they have any idea what diagnostic tests on such things cost.
call these specialists, be clear about your lack of insurance and say that you have cash in hand. sometimes, they will even ask for a deposit up front. find out what it will cost for a consultation. if you can afford it, schedule one.
make it clear to all office staff and health professionals you see that you will be paying yourself. a consultation should not set you back too significantly. when there, you can ask the specialist whether he has a better idea of how much the diagnostic tests cost. ask about any discounts you can get as an uninsured patient. they do offer them, but may not be able to tell you offhand what anything costs without the billing/accounting person weighing in on it, so you may have to call back to find this info out (or be emailed).
if the costs will be prohibitive, that is when you consider signing up for medical coverage. try to scope it out as much as you can yourself in advance.
this is the only kind of ‘shopping around’ one is really going to be doing in this so-called -healthcare system-.
((we’ve been having to do this for the last year for my partner, who does not have nor want coverage and probably won’t exceed the out-of-pockets on a policy even if he did have it. many doctors are willing to work with him and help him to find out and manage costs, but some won’t even see you without insurance coverage and a referral))
The seduction of the “market efficiency” trope is pretty strong for a lot of policy advocates. And it was such a loud part of the Reagan-Thatcher years that a lot of the public got sold on it as an absolute truth. And in order to get Democrats back into the White House during the Poppy Bush years, the DLC adopted the idea that public-private partnerships could allow the market to work its magic with the assistance of the public sector. You just have to look at Chicago’s school system to see how wrong that idea is.
Patients aren’t consumers because providers don’t want to show their prices and allow comparative shopping. In most cases illness creates a cost that makes a patient value immediate care over less-expensive care. There is no way to force a market bargaining situation on that relationship. It fundamentally corrupts a doctor who is checking the clock because of his profitability quotient, whether it is his desire to do so or is forced by a medical system CEO.
Also, if health care is to be the right of all then a market that discriminates against people with the ability to pay (the very definition of a market) is going to leave some people out. It becomes the cruelest form of rationing.
Quasi-market systems to serve public purposes is a chimera. Whether cap-and-trade, Obamacare, charter schools, or toll roads, the transaction and administrative costs are either too high or the service is held to an indequate level.
Let us now lay that one to rest across the board.
“In most cases illness creates a cost that makes a patient value immediate care over less-expensive care. There is no way to force a market bargaining situation on that relationship.”
You’re right. Hmmm…. what would be a more powerful and efficient way to bargain with health care providers? What large entity would be able to do such a thing? I wonder.
Well…if you want the biggest community risk pool possible, maybe that organization should be the World Health Organization. The only wrinkle is how to finance it.
Short of that, of course, is Medicare/Medicaid with Long Term Care Subsidies For All and a community risk pool of 300+ million people. Or you could go the UK route with VA Healthcare for All (VA already does long term care).
I remember a chart that shows very clearly that US healthcare costs skyrocketed with healthscare companies joining in on the NYSE. And, let’s face it, the shareholders must be fed and appeased with money every quarter. Then let’s not forget CEO Maguire of United Healthscare who was making $125M yearly. What a horrible joke on those ‘consumers’, eh! Since that scandal, the executives now get hidden money, especially in stock, but also lots of other things…like mansions and planes and yachts, etc. Then, of course, there is that ever-hungry monster, called political campaign chests and millions upon millions go into those chests (legalized graft) every month/year to insure the permanency of private health care in this country. Cutler is obviously being paid well to dispense his propaganda.
I’d love to see that chart.
typo in article David Cabot should say David Cutler
Ah yes. “The Cutlers speak only to God.”
Meanwhile, Orry-gone is hiring 400–yes, Virginia, that’s FOUR HUNDRED–temps to manually register the state’s new consumers of crappy, over priced medical insurance.
This article from Atul Gawande describes what happens when you actually treat medicine like a business and profit center – exploding costs. Unlike someone trying to sell me an expensive car, I am in no position to say no, evaluate what really needs to be done to me, and what it should cost.
http://www.newyorker.com/reporting/2009/06/01/090601fa_fact_gawande
We license doctors and most health professionals because we know the average person cannot evaluate the expertize of the practitioners. We license drugs and medical devices because we know most doctors can’t evaluate the efficacy of the materials without carefully controlled and monitored trials.
The free market is great for cars, clothes, and TVs. It is not good for medical care.
am i wrong here? i thought that built into the definition of ‘free market’ meant free to enter/exit at will.
with your health, the only way you are free to not participate is if you are willing to die, if those are the consequences.
this is not freedom to participate at will. you will not die if you don’t get a TV, car and any commercial good except food, sometimes shelter, and generally sanitation. your life will be different, but you won’t run the risk of losing it for things that could be readily solved by skilled professionals>*
*who should be comfortably compensated under ANY system. hey, let’s talk about the quarter million dollar education cost. how much of that is truly necessary?
When I hear ‘skin in the game’ I immediately think of HCA.
Over the last 30 years Hospital Corporation of America has had multiple private equity buyouts – buy the company, give yourself a huge dividend, pay for the dividend with huge debt , sell the company.
And so HCA must aggressively push prices to pay for this debt. In this game , the patient at HCA is going to get skinned.
Obama & Harvard health minions want patients to be “consumers” “shopping” in “marketplace” for the “best price”. Are these people demented? No, not really. Just crazy like foxes, seeing patients as hens to be bled.
http://patriceayme.wordpress.com/2013/11/15/obamacrap-trade-plutocracy/
The only people who “shop” their health care are people with jobs and money. You can’t get Obamacare without showing your tax returns in my state, and we had a severe foreclosure problem.
In the US, stem cell cures are still at the research level. In Canada, they’ve been using them as regular cures for 20 years to spectacular effect, and for the cost of three lab visits to create the stem cells from your own blood and then a week in a hospital sterilized enclosure (like a clean room around your bed). My friend watched a friend of hers recover within two weeks from stem cells used to replace his entire blood stream, a process that took less than an hour in the operating room. A bone marrow transplant had failed; the 6’5″ man weighed 110 pounds; couldn’t walk; no hair; told to write his will. Two weeks after treatment my friend didn’t recognize him at the local co-op. He was ambulatory, color in his cheeks, and his cancer has been in remission for over 16 years. I called the guy’s wife four years ago to verify this story. The biggest cost, covered by Canadian health care, was the week in the hospital in a bed gerryrigged with plastic sheets around it.
I asked a 33-year-old Canadian doctor why he didn’t move to the US to make more money, and he sneered at me. He said, ‘We practice medicine here, not marketing. You couldn’t pay me to work under the American system. I grew with Canadian healthcare. it works. I took a Hippocratic Oath to help people, an dI get to do it daily’. This kid also volunteers two nights a week, in addition to his regular practice, to help in hospital emergency rooms to keep his triage chops up.
I asked him if he was unique or was that thinking common among doctors there. He said maybe the older doctors on the verge of retirement are resentful that they didn’t move to the US decades ago, but not among his generation or Gen-X. He said we view American healthcare with disdain. He said the Americans haven’t come out with any medical breakthroughs in decades that we haven’t already discovered. He said you don’t know about it because your press doesn’t cover it, and you mock Canada as your broom closet. He snorted and said your NIH scientists are still working on some things we’ve already put into practice, no wonder they get the money for their research.
Indeed, the whole medical system form docs to hospitals is mainly corrupt and for profit. Every part of the system is infected just as every part of American society is infected with it. The U.S. media is nothing but propaganda and PR and should be ignored on every issue–as I like to say, everything the mainstream says is a lie–even when it’s true.
they want us to pay a ton of money, hardly ever use the ‘service’, and then die as soon as we can.
the end.
how much of this healthcare is invested in by the same corps that spew manufactured food? enquiring minds want to know!
“So how did Cutler get involved in such an intellectually and morally corrupt endeavor?” Well, he’s from Harvard, that’s a start.
And this new deal is not an experiment, or the only experiment aspect is whether and how greatly it will further enrich the medical insurance industry. As for us, the victims, the H boys couldn’t care less. You need skin in the money game to be relevant.
There’s a single nugget of accuracy in Cutler’s doubletalk and airy-fairy.
“The first one is because the administrative costs of running our health care system are astronomical.”
However, he then goes on to lie by silence.
Health insurance is an administrative function for health care. It’s got no other purpose that taking money, holding onto it, and then cutting checks. That is office work, nothing else.
And since it’s mostly private health insurance, its administrative costs include profit, breathtaking salaries for ‘C’ levels, and a whole lot of friend money for the people who run governments. Along with positions for girl and boyfriends, sons and daughters, etc. Lot of lawyers, since its venue for collection is civil court. And the newest in headquarters. Always new headquarters. Privatization at its finest.
Because acknowledging insurance companies and perhaps the largest sink hole in the delivery chain, Cutler preserves his access to private money. Or at least, his access to the MSM.
Last night on Wisconsin PBS there was a presentation on the Affordable (to who) Care Act. The telling question from the audience was “What happens in months when I don’t have money to pay the premium?” by a woman who looked like she had little….
I think there’s just one kind of folks. Folks.”
― Harper Lee, To Kill a Mockingbird
“Are these people demented?”
You know they are; and the nature of their insanity is that their moral sense has atrophied into misguided consequentialism informed by false and moral bankrupt neo-liberal ideology.
“Are these people demented?”
Of course not, they are criminal. We are way past the point where elites like Cutler can hide behind the excuse that they believe what they believe in good faith and that, at worst, they simply mistaken.
Obamacare trades upon the lie that universal insurance is the same as universal care. The two could not be more different. Universal insurance is simply a mechanism to loot.
It may have been mentioned by someone else, but Cutler justifies the high cost of health care in the US by repeating the talking point that the US medical system is good at acute care, and acute care is more expensive.
Let us examine this point. The truth is that the American healthcare system needs to be good at acute care because it sucks at general health care. Tens of millions of Americans with no insurance or crappy insurance or no or crappy access to health care don’t get the basic care they need early on so that health crises can be averted.
But even basic preventive medicine is much more expensive in the US than it needs to be. Patients in the US pay much more for the drugs they need to treat chronic conditions, even when they can afford to see physicians. And lets face it if an acute event occurs, the outcome often depends on which hospital one is taken to and who is on duty.
And yes, the costs associated with this acute event are astronomical but that is because hospitals use fantasy billing practices where a patient receiving a few Tylenol might be charged a hundred dollars for them. When the whole bill looks like that, a hospital visit that should cost a few thousand at most can suddenly morph into a hundred thousand.
And that is American health care. Insurance companies make money by jacking up prices and restricting usage. The medical industry and Big Pharma make their money by jacking up their prices which both restricts usage early on creating a reservoir of acute events and then bankrupting those who have them. From where I’m sitting, it is all looting and criminal, and whatever you want to call it, the one thing it is not is care.
Actually, as I read when reading a historian (can’t remember who it was), American HC is good at acute care because of the constant wars we’ve fought for decades thus the preponderance of surgeons and surgical procedures which dominate medical care in place of preventive care. The guys who were in MASH needed civilian jobs right?
I don’t see people like Cutler or other political operatives as bad people. I’ve met these kinds of people in Washington over many decades–I don’t enjoy their company, for the most part, but they view things from an angle that is foreign to us. Politicians (Cutler is one) are power-brokers, not moralists or philosophers nor benefactors. They deal with political reality. I always view it, as I’ve said many times, as table with mafia dons with guns on the table all negotiating on the basis of their firepower. Politicians try to get these gangsters to come to an agreement about who controls what territory without going to the mattresses. The scene in Washington is very polite and bland on the surface but the big-shots are brutal and will stop at nothing to get what they want. I’ve known known some of these people and known wise-guys (I’m part Italian) and they are the same just with college degrees.
What the left doesn’t understand even now, is that if they want to come to that negotiating table they better be armed–and by armed I mean with political muscle. I can go further about what is means but few people are ever interested in that preferring to just shake their fists at the evil oligarchs and get mad at me for even bringing it up.
Nice charts–particularly the top one, however they are seriously out of date–but the charts look essentially the same now as they did then. Where were these charts during the HC “debate?” Why didn’t progressives insist as a precondition for supporting Obama’s efforts that we deal with facts not theory and fantasy as was the case? The left lost the struggle the minute it accepted the terms of debate Obama and the mainstream outlined. As you know I have blamed the left/progressive community as much as the Obamabots and the RP for this mess.
“Where were these charts during the HC “debate?” Oh, single payer blogs…
Of course, in the ghetto we knew all that but it did not get into the mainstream media.
Make it simple for the simple.
Why not do the MATH?
Is it because ALL journalists flunked math?
Of is it something else!
Try dividing the Nations Expentiture on Health Care by yhe population and then write about that number!
NO ONE does because NO ONE in AMERICA can handle that truth!
Including the Journalists!
And EVERYONE wants someone else to PAY!!!!!!!!!!!!!
Corruption continues to define the Business Party – All republicans and All democrats playing the voters for the fools we continue to be!!!!!!
There is another element that distinguishes the US from the other countries on the charts above. It is the one of the few countries that treat HealthCare as privatized. Most other developed nations have largely, but not uniquely, healthcare coverage that is universal and delivered by a National Health System (NHS) – meaning a government agency.
When the list of countries is restricted to the OECD, the per capita costs clearly shows the US at the highest – see here. Why’s that?
Because an NHS mandates (price-fixes) the fees of HC-practitioner services including fixed hospitalization costs, thus capping them.
But what Americans perhaps do not understand about their privatized healthcare costs is this: That because they work and have a company or (local, state of Federal) agency pay for it, it’s “free”. AbraCadabra!
Which is clearly not so:
**A private company purchases the coverage from BigInsurance. But it recuperates the cost how? By imputing the insurance policy cost in its operational overhead and recovering it within the pricing of its products/services to customers. So Americans pay for their healthcare insurance each and every time they go shopping. Whether they benefit from healthcare insurance or not.
**If the service is provided by a government entity, then obviously HC-insurance is paid out of taxpayer revenues. Again, we all pay for it out of our incomes.
Which are two good reasons why healthcare should be provided as universal by an NHS – just like policing, firefighting, or National Security. That is why most modern countries have an NHS, and why we should have one as well.
ObamaCare is a necessary evolution in our archaic and unfair healthcare coverage. But it remains a palliative compared to other developed countries with a National Health Service.