By Lambert Strether of Corrente.
I wouldn’t have imagined two or even one year ago that Senator Bernie Sanders would introduce a Medicare for All Bill with sixteen co-sponsors (highlighted below). Here’s the cover page of the bill, just for the happy dance:
(Shaheen and Whitehouse came on board after the bill was introduced, so they don’t appear in this image.) Frankly, I’m so unused to good things happening that I’m a little bit gobsmacked, and don’t know quite what to say!
In this post, I’ll look briefly — and probably simplistically, because I’m gobsmacked — at the politics of the “Medicare for All Act of 2017” (“BernieCare,” as I suppose we must call it). First, I’ll look at the co-sponsors; then, I’ll look at the coverage, and lastly, I’ll look at funding.
Politics of the Co-Sponsors
First, I looked at the co-sponsors of the bill, to see if they had, as we say, “skin in the game.” In one important sense, they do. From MapLight:
Democratic Holdouts On “Medicare For All” Have Received Twice As Much Insurance Industry Cash As Sponsors
Democratic senators who haven’t signed on to Sen. Bernie Sanders’ “Medicare for All” proposal have received twice as much cash from the insurance industry as the bill’s sponsors, MapLight has found.
The insurance industry has donated an average of $23,600 since 2010 to senators who have co-sponsored Sanders’ bill, according to a MapLight review of campaign finance data compiled by the Center for Responsive Politics. Democratic senators who have not yet supported his legislation, including Sen. Angus King, a Maine independent, have received an average of $55,500 from the industry.
So, the 16 co-sponsors are leaving money on the table. Moreover, they’re risking the insurance companies (and perhaps health care trade associations, and Big Pharma) funding their opponents. The co-sponsors are indeed taking a risk. But how big a risk? Consider the following table:
Table 1: Political Risks of Medicare for All Co-Sponsors
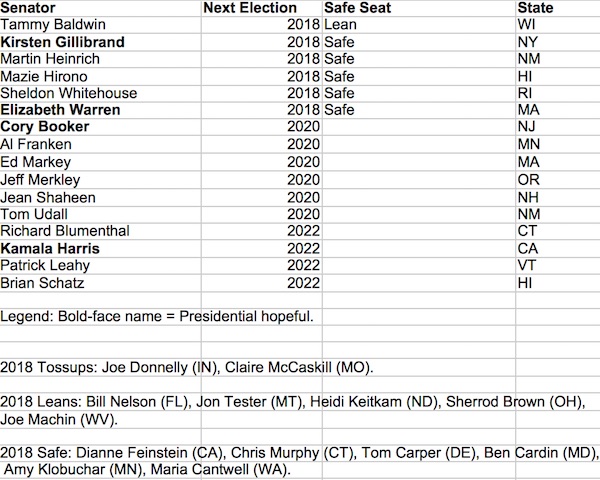
(The data is from 270 To Win, whose “Safe Seat” evaluation is from Larry Sabato.) From the table, we can see that only one Senator — Tammy Baldwin — is putting her “Leans Democrat” seat at risk by endorsing BernieCare; all the Senators either have safe seats, or are not up for election in 2018 at all. We can also see a gaggle of Democrat liberals in safe seats — looking at you, DiFi! — who don’t support BernieCare, presumably because markets. And we can see some leans in the Swing States, especially Sherrod Brown, who may perhaps doubt their ability to sell the bill (oddly).
I’d argue, then, that the 16 co-sponsors have concluded that the left finally has real power in the party; that is, “they have no place to go” is no longer operative (as indeed it would not be with Obama voters flipping to Trump, Sanders voters going for Trump, voters staying home, and pressure from the left from Our Revolution and DSA). So for these 16 Senators, there’s no downside in appeasing the new power. The New Yorker’s John Cassidy writes:
And, as a number of progressive groups have already expressed support for the Sanders bill, anyone looking for their support in 2020 would be taking a risk by not falling in line.[1] A poll taken during the summer by the Kaiser Family Foundation indicated that sixty-four per cent of self-identified Democrats now support a single-payer system. A more recent survey from Gallup produced similar results. These are the voters who will decide who wins the Democratic primaries.
(Yes, poll results vary by the question. It’s up to the political class to structure and drive the questions.) I’d speculate that if Jon Ossoff had won his race in GA-02, we wouldn’t be seeing this. The Ossoff race was, in essence, the beta test for a Clinton campaign in 2020 except without Clinton: Media-driven, appeal to wealthy suburban Republicans, “Just look at the other guy,” enormous amounts of spending, mushy centrist politicies, and throwing the left under the bus. Ossoff was, of course, against single payer, and Sanders called him out for it. Had Ossoff won, I don’t think BernieCare would have its 16 co-sponsors. But Ossoff failed, as did Clinton.
Of course, that doesn’t mean that the co-sponsors are “sincere,” as clearly Sanders is, but I don’t see that as bad. If opportunists like Booker see BernieCare as an opportunity, what’s not to like?[2]
Politics of the Coverage Provisions in the Bill
Now I want to call out a couple of provisions in the bill. As far as those covered:
Moreover, during the first year, every child between the ages of 0-18 would become eligible to enroll in the Universal Medicare program.
Besides being the right thing to do, enrolling children immediately is politically very smart; it “builds on” the ACA, which allowed children to extend their coverage on their parent’s policy. So why not cover every child, without reservation? Second, for those families who are provided with this universal concrete material benefit, it creates the endowment effect that ObamaCare benefitted from in the fight against repealing it; it’s going to be hard to roll back the program when children already benefit from it; and it’s going to be hard not to keep rolling it out when people can see the benefits in their own families.
- Hospital services, including inpatient and outpatient hospital care, 24-hour-a-day emergency services and inpatient prescription drugs.
- Ambulatory patient services.
- Primary and preventive services, including chronic disease management.
- Prescription drugs, medical devices, and biological products.
- Mental health and substance abuse treatment services.
- Laboratory and diagnostic services.
- Comprehensive reproductive, maternity, and newborn care, including abortion.
- Pediatrics.
- Dental health, audiology, and vision services.
First, ZOMG!!! Dental!!!!!! Besides being medically bad for you, poor teeth are a class marker that make it hard to get a job. I don’t think the Acela riders know what a huge difference dental would make in the flyover states, out in the colonies. To me, this is huge (and an obvious vote-getter; who wants to depend on charity or the ER for dental care? So pay attention, Sherrod!) Second, the more complex issue of abortion provisions. From ReWire:
Under Title VII, “Universal Medicare Trust Fund,” the text of Sanders’ bill appears to reference Hyde as one of the “restrictions that shall not apply.”
Specifically, “any other provision of law in effect on the date of enactment of this Act restricting the use of Federal funds for any reproductive health service shall not apply to monies in the Trust Fund”—meaning that Hyde couldn’t apply to Medicare funds.
Another section of the bill includes “comprehensive reproductive, maternity, and newborn care” within the scope of Medicare for All’s coverage. Reproductive rights and justice advocates in August told Rewire that it’s just as important for universal health care proposals to spell out abortion care within the scope of covered services as it is to end Hyde. Their consensus now is that the bill’s “comprehensive reproductive care” includes abortion care, and they praised Sanders for it.
“Insurance coverage of abortion is critical to ensuring women can access the services they need, helping to protect women’s health and economic security,” Rachel Easter, the National Women’s Law Center’s counsel for reproductive rights and health, said in an email.
That recognition emerged during the drafting of the bill, which was “written to cover abortion, explicitly,” a Sanders staffer told Rewire Editor-in-Chief Jodi Jacobson.
From a purely political standpoint, one can only wonder what Clinton supporters who were able to swallow Clinton’s “never, ever” on single payer feel about abolishing the Hyde Amendment (which the ACA did not do, as Obama signed an Executive Order making sure the Hyde Amendment applied to Federal subsidies in his signature legislation). I’d think they’d get on board the BernieCare train immediately, but what do I know?
Politics of the (Lack of) a Funding Proposal
Finally, BernieCare has been criticized because it lacks an explicit funding mechanism. VT Digger:
Observers said that the lack of a clear funding mechanism is a major weakness of Sanders’ new bill.
Gerald Friedman, an economics professor at the University of Massachusetts who has worked with Sanders on this issue, said that though he sees it as positive that many senators are getting behind single-payer, it is not very meaningful without a funding plan.
“Honestly this is not serious,” Friedman said. “It’s a bumper sticker that ‘We want single-payer.'”
Without a proposal, he said, critics will say that Sanders is not serious about the proposal, that it’s so expensive that supporters don’t want to discuss it, or that proponents couldn’t come up with a way to fund it — which, Friedman said, is not true.
“If you put out numbers, you’ll be criticized,” Friedman said. “If you don’t put out numbers, it’s even worse.”
(As far as Friedman’s “not serious” comment, I hope you are convinced from the rest of the post that BernieCare has been carefully crafted to achieve the ends it achieved. Another way of saying that is to ask: “Would sixteen Senators have signed onto the bill if the funding mechanism were there?” I think the answer is no.) I disagree, for several reasons. First, Friedman is wrong; the Sanders white paper that accompanies the bill proposes several serious options. Second, when making a sale, the price is part of the close. You don’t lead with it (unless, I suppose, that’s your only selling point, which is not the case with BernieCare). Third, the whole “PayGo” discussion, by design, is a recipe for setting winners and losers against each other from the start, which isn’t a recipe for passing the bill. Fourth, as MMTers know, the political class doesn’t understand how taxes work anyhow. If straightening them out is prerequisite for passing the bill, we’ll never get anywhere. Fifth, this is an objection that can’t possibly be made in good faith: Every other industrial nation has been able to afford universal health care, and several have adopted the single payer approach; last I checked, Canada hasn’t collapsed from fiscal exhaustion induced by funding its Medicare program. So we can do it. Let the detail people figure out how.
In summary, I think it makes very good sense to take an approach programmers call “separation of concerns”; separate what the bill can do (save hundreds of billions of dollars and thousands of lives) from how to pay for it (a Beltway discourse that has any number of pathologies). And if there are any wonks out there who operate in good faith, they’ll be getting on the BernieCare train by proposing funding mechanisms themselves, instead of whinging that Sanders didn’t pick one.
Conclusion
In summary, BernieCare could be said to be aspirational; after all (even though a reasonable number of Republican voters support Medicare for All, too) the bill won’t pass this year or even next year. But I’m amazed and happy to see that single payer is finally “on the table” in the Senate, after Obama and the career “progressives” successfully kept it off the table in 2009. For the next few months, at least, that’s victory enough. In my next post, I’ll take a more detailed look at BernieCare as policy.
NOTES
[1] As Ian Welsh wrote: “The left must be seen to repudiate Obama, and they must be seen to take him down. If the left does not do this, left wing politics and policies will be discredited with Obama.” That didn’t happen with Obama. It did happen with Clinton.
[2] Of course, there’s always the scenario where the Democrat establishment, having hazed over the distinction between Medicare for All and “universal health care,” conclude with a sigh that BernieCare is such a “heavy lift” they can’t pass it , and “reluctantly” go with some horrid bipartisan compromise, hoping to kick the can down the road for another eight years like Obama successfully did. But politics ain’t beanbag! If the left has real power, betrayals will be seen as punishable, even by opportunists. (In retrospect, it was good that the left roughed Booker up on his pro-Big Pharma vote on drug importation.)


This is great. It will be attacked by the right and center, which means both parties will loudly proclaim it is far too expensive and can’t be done. It may bankrupt us all. I wonder where Hillary and Obama will fall on this proposal. They could help it along, if they get on board.
I thought there was a proposal to charge a payroll tax on corporations somewhat equivalent to what they now pay on their employee health care. That would make it easy to exchange their current Aetna card for a medicare for all card. That tax seemingly would fund a good deal of this, given that the federal and state governments already pay a big slice of the cost. But I agree, once you lock in the funding mechanism the games begin.
> It may bankrupt us all.
The currency issuer can’t go bankrupt.
I can see plenty of money opposing this. It will be easy for opponents to assume current costs (price gouging from all the snouts in the trough (clinicians, C suite admin and ceos, pharma, insurers, banks, private equity…) would continue. So, how is this to be paid…easy to see how people could come to fear change – the media is very good at doing this.
Under single payer, it’s the central government that determines the price a doctor would receive for a 15 minute visit from the public purse. Don’t like the price, then… well, I hope you get the picture.
It leaves only the private, for profit hospitals and a much smaller medical insurance sector to cater for those who can afford to leave the public system (to jump queues for example)
Thanks NC for keeping us all informed
The Sanders bill, unlike Conyers’s HR676, doesn’t seem to require hospitals become non-profit. Presumably he saw how the hospital groups leaned on Obama and decided to avoid that, at least for now to get some other senators signed up in theory.
…wife is R.N., Europe-“single payer”; there is choice involved, whereby one can choose whether to utilize private, government, or other form of healthcare provision…private and government provision utilize often, same hospitals-facilities…
Without choice of retention of U.S. workplace provider (and workplaces will end provision at some point if national care is provided), and private insurance-healthcare, we see the issue easily propagandized by health profit industry, and bought and sold government representatives.
Also Europe, education of doctors-nurses is based upon payback of years Ed., in public hospital service at diminished rate. Government apartment complex are available for new employees, “paying back” years of education…
…commonly known as a social system…
Costs vary, but are generally half those of U.S. health profit…
why even allow them to leave the public system? Or basically ban everything else except for purely cosmetic procedures pretty much.
Not quite … if we accept some finite liquidity issue per annum …
We have to choose between guns and butter. If we choose fewer guns, we can have more butter. This is the choice LBJ, and every other corrupt politician refuses to make.
A totally rubber currency doesn’t help, one is simply increasing the number of zeros, not the actual purchasing power. Unfortunately part of the false prosperity of the US is the unnatural advantage the US dollar, as the primary world currency, gives us. If the US loses the Petro-Dollar advantage, we will have to make do with a lot fewer guns and butter both ;-(
Venezuela, unlike Greece, has a sovereign currency, but it doesn’t keep them from mismanaging themselves (in an adverse oil market) into the toilet.
I’m not so sure that was the problem that LBJ had. As I understand it, he could’ve had both guns and butter, but he would’ve had to raise taxes to do so, in order to keep inflation in check, which he didn’t do, for political reasons.
The problem Venezuela has is that they peg their currency to the dollar, giving up the advantages of a sovereign floating currency. Plus they have have saddled themselves with debt in a foreign currency. If they understood MMT they would have avoided these mistakes and would have more fiscal flexibility.
Its not guns vs butter. Its figuring out how to reduce the cost of butter to pay for the guns.
If the US can figure out how to reduce the per capita cost of healthcare by a third, the savings would equal the entire US military budget. Cutting costs by a third sounds impossible, but it would still leave us as the most expensive healthcare system in the world except for Switzerland. Is there anything else at all where we are more expensive than Switzerland.
Every other developed country in the world has figured out how to be substantially less expensive than the US. Why is the US unwilling to understand this?
http://www.visualcapitalist.com/u-s-spends-public-money-healthcare-sweden-canada/
Cost is the primary driver. Pass laws that reduce costs substantially. Everyone pays the same price–a number based on the large purchaser status of the US economy–is a start. We should pay the lowest collective healthcare prices on the planet given our bulk purchasing and the amount our taxpayers plow into basic research.
No, of course, we won’t go bankrupt. But do you think that will stop the accusation, we are going bust from this. It is far too expensive. Heavens help us, tax and spend democrats making us bankrupt.
we are going bust from this. It is far too expensive
I think that’s pretty much what the general population is saying about medical costs.
Whyizit that when people talk about the cost of MFA/Berniecare they fail to mention that those very big insurance premiums and co-pays free up a lot of cash that could be moved over to Medicare payroll deductions – and probably for less than workers’ current payroll deductions for health insurance. Thus, it seems like that alone would make this revenue neutral – or did I miss something?
Opponents that are in or are shilling for the insurance industry want people to think that payments for a public insurance system are taxes, not premiums. Once people realize that their premiums would stay the same or be less, for a better service not tied to their employer, they would obviously prefer the public insurance system.
If they want to call premiums a tax, then I’m sick of being taxed by a private entity whose business model is denial of care.
Eliminating the insurance middlemen siphoning off their administrative costs on every transaction will free up funds for productive use, more than paying for the bill.
There will be there usual attacks from the right, but most important will be negotiating with the left (while celebrating it as essentially boosting the discussion, neither PNHP nor the HR 676 folks (Health Over Profit) have endorsed this).
Those of us doing grassroots M4A are now having to provide education on two quite different plans since a huge chunk of the savings to pay for single payer depended on eliminating multiple bureaucracies which Sanders’ plan doesn’t do.
We are scrambling to find and create new materials to reflect the current reality.
Most problematic is that a public option was written into Section X of the bill by Kristen Gillibrand. For some, that means it’s built to fail.
Looking on the sunny side, right, we’re not at the finish line. This gets the conversation going in a big way.
There is an excellent debate between Margaret Flowers, MD and Jon Walker who authored of the ShadowProof proposal, which follows a long-ago approach recommended by Jacob Hacker which has been dismissed by the single-payer community for preserving private insurance (so multiple payer) and copays.
Long but provides an excellent review of all the issues. Decide for yourself!
https://www.singlepayeraction.org/2017/09/05/jon-walker-and-dr-margaret-flowers-debate-the-road-to-single-payer/
Thanks for the link. Here’s a recent update from PNHP that includes areas for improvement of the Sanders bill, and a form to submit questions for a Q&A with Dr. Adam Gaffney Tues. 9/19 9pm Central.
This is really good, thanks.
If I’m reading Section X right, it doesn’t look like a bad idea to me at all. Allow ppl to buy-in before the Medicare age is lowered to their level? I assume that’s to get them hooked.
Thank you for the link!
The involvement of Jacob Hacker, one of the primary architects of the Clinton healthcare fiasco in the nineties, should set off red flags and sirens. And Walker has spent quite a bit of time helping lay the groundwork for an anti single payer campaign. I couldn’t say whether there is any formal coordination going on, but the intent is clear enough. Walker has done a lot of posting at BalloonJuice, formerly a dedicated right wing site, now turned Clintonite.
Sadly, if this issue starts to develop real legs, we can expect a lot of false flags and sympathy trolls. I’m glad to see advocates like Flowers staying ahead of things.
Having now listened to the podcast, I’m experiencing a lot of deja vu. Walker’s stance is a regurgitation of Bill Clinton’s “Pay or Play” campaign rhetoric from 1992. It’s ironic that Jerry Brown, who ran as Clinton’s primary opponent on a single-payer ticket, is now in the opposition camp, but state-by-state efforts are futile anyway. Those who are old enough may recall that one of the explanations advanced for the failure of the Jacob Hacker/Hillary Clinton plan was confusion from the number of alternate proposals put forth by other Democrats.
There is an underlying resistance in the cost analysis, “you can’t pay for it” argument. That argument is, “to make Medicare for All work, you will need our cooperation and willingness to NOT fight this in any way we can, and we cannot promise that. Our one hope, if this is passed, is to pull out all stops to bury it under a legislative avalanche, a financial tsunami, of restrictions and non-cooperation locally, wherever we have power to do so.”
While the bill is setup to stop the first line of attack (Hyde Amendment), there will still be a medical/political establishment in full place ready to win back its privileges, one that is not averse to publicly showing its criminal underwear in public. That is, IF this bill is passed, AND the public is not mustered into an all-out fight for it. Be ready for a true fight, prepare the public for all the counter-arguments, and prepare to battle in the regulatory bureaucracy for enforcement, and MAYBE this bill can win if reintroduced if it fails this time. Of course, a political revolution that gains more power in state and central government would guarantee its passage and enforcement, but we can’t have everything, can we?
I do have a question: what’s gonna happen to all those medical insurance and processing employees after BernieCare becomes law? They’re gonna lobby against this.
Sure, we could assign them to build a highway from St Louis to Santa Fe, but that’s temporary.
Both the Conyers House bill and the Sanders Senate bill contain provisions for insurance industry workers. People who support a Medicare for All universal insurance system should consider this issue and evaluate these provisions.
To better determine the impact and identify further solutions, we need an analysis of this workforce. That would include whether these are US workers (as opposed to offshore or H1B), normal attrition rates, potential merger/acquisition related layoffs, availability of jobs elsewhere in the insurance industry, expected job openings within the expanded public insurance system, and people currently working only to have health insurance.
In the larger picture, there’s tons of work that isn’t getting done because of austerity, offshoring, downsizing, and the general failures of our economy. There should be plenty of work available, project-specific and permanent, for people in every region, with all levels of skill and interest…..but that’s another discussion.
Notes:
2016 – BCBS layoffs and outsourcing
2015 – Aetna: Discussion of potential merger related layoffs
Great response, Mary. Thanks. (IIRC, you were a pup in the FDL days?)
I personally have an aversion to putting too many restrictions on this. If they lose their job, it sounds like severance to me, not did you get another job or do you have a visa. This is a one time payment and hopefully it will block any strong opposition.
Mary…
Doing real work for real good.
Thank you.
They will be working in the new coal mines and building the border wall.
If you look at the Canadian system, there are still insurance companies for the employer-provided or individually-covered components, such as private hospital rooms, pharmaceuticals, dental, and foreign travel insurance. But they are a much smaller percentage of the system and the doctors’ billing departments are tiny compared to the US. I don’t think the doctors are going to have an issue with that.
Not to be rude but I didn’t see anybody too concerned about automation when it comes to the trucking industry and the 10 million people it employs.
Oh right that’s blue collar workers sorry.
well just like the U.S. healthcare system is an inefficient system (in terms of cost for what we get), trucking is inefficient compared to trains (in terms of fuel use). Just the way it is. Trains for the win.
In addition to opposition from insurance companies I expect Big Pharma, the hospitals and the physician and dental lobbies to oppose any plan that will impose cost controls on them. In addition to scaremongering about taxes I can see people freaking out when they gets calls from their doctors saying that they will be forced out of practice if Medicare for All passes. People hate insurance companies but hold doctors in high esteem so this could be major problem.
When talking about doctors’ role, prospective or actual, in the problems afflicting American health care, it’s really important not to treat them as a monolith.
Surgeons and specialists making big salaries for procedures that can’t be outsourced and a minimum of paperwork are going to resist this.
The far more numerous medical doctors, including PCPs and family physicians, whose professional lives have been reduced to a fury of timed-to-the-second patient interviews and out-of-control paper chases, with essentially no independent say in the actual delivery of care to their patients, and salaries that in many places are being cut for failure to keep the rising pace set by corporate bosses, are coming around to single payer in droves.
This phenomenon has been chronicled with some frequency of late here on NC, see for example “A new survey says doctors are warming up to single-payer health care” (from NC Links 8/20/2017, just a few weeks ago):
https://www.statnews.com/2017/08/17/doctors-single-payer/
“Fifty-six percent of doctors registered either strong support or were somewhat supportive of a single-payer health system, according to the survey by Merritt Hawkins, a physician recruitment firm.”
My conversations with folks in the medical community around Boston lead me to believe these results are accurate. I think there are more allies in the push for single payer than is widely realized; I hope this legislation is going to start drawing them into the sunlight.
The ER physician that brought my son back to life (effing fentanyl) supports single payer and gave money –far more than $27– to Bernie.
When the first single-payer plan was established in Canada, in the Province of Saskatchewan, in 1960, the doctors went on strike. For two weeks. They failed to stop it – because the CCF (Cooperative Commonwealth Federation) was led by a fighter – Tommy Douglas. He shamed them back to work, with the support of most of the people of Saskatchewan.
About that — comparing with efforts in California, how did Saskatchewan deal with the budgetary effects of Medicare during recessions?
See here.
“. . .universal hospital insurance which was introduced as early as 1947, and by 1958 had been adopted nationally as a federal-provincial jointly funded program.”
I think that answers your question as the federal government agreed to help fund the program and a sovereign government does not run out of money.
How much of the money currently going to for-profit medicine is being hoovered up by the administrative layers? I wonder if doctors wouldn’t take as much of a hit as some might think. Some of them might see it as an acceptable trade-off, if it means that they don’t have to deal with those administrators.
Over 20% of US medical costs are administrative – v. LESS than 1% in Canada’s single payer plan.
The formal estimates are low, since they don’t capture the time that MDs spend fighting to get claims paid, and that is relatively high priced time. Some estimates put total admin costs at over 30%.
Also not included is the time and aggravation for patients and their families who have to submit claims to their insurance co’s. Here in Canada we don’t even see the bill, the physician or hospital bills the provincial plan and gets paid with none of the customary reluctance that I have seen from US insurance co’s.
I was shocked at the ordeal that my dad went through getting the costs of my mother’s final illness paid. First of all, that there were so many separate bills — ambulance service, prescription drugs, therapists, and lengthy itemized bills from the hospital. Then there was getting the insurance company to pay — the process of submitting insurance claims, then having to get the ones that were denied (there were always some) clarified with the issuer and resubmitted, sometimes more than once, and some never paid. It was downright adversarial and very hard on my father, who was already devastated.
I don’t trust the Democrats as far as I can spit. Of course these co-sponsors would sign onto a bill that has no chance of passing this session. They can afford to be for it now until they’re against it later when it could pass, such as if they succeed in convincing us to vote in more Democrats instead of taking a chance on a newbie Green, Independent, or third party who has a 5% chance of winning against incumbent Democrats due to the huge financial power of incumbency, and being part of the Machine.
No, this is a win-win for Dems and a toss-up at best for the rest of us. Forget 3rd party candidates winning now. It will be “We can’t risk *UniCare if Dems don’t win” for the foreseeable future, especially now that ‘Supreme Court!’ isn’t the rallying cry. *UniCare meaning Universal Medicare
Even if they succeed in getting more Dems elected, there’s nothing to stop them from pulling an Obamination. Obama was for single payer before he took it off the table, and he was for Social Security before he strapped that poor lamb down on the sacrificial altar of his Grand Bargain. Thank God the Tea Party rabble rousers effectively, if not wittingly, saving SS. Bait and switch and breaking our hearts is not beneath the Dems. They have no shame as long as their corporate donors are satisfied.
Until the Dems seriously address how the defense/security budget to maintain a global empire for Capitalism is sucking the life blood out of the country and budget, there will be no UniCare. They should tell the truth about that exorbitant expense and how we need to balance vital interests, not based FACTS NOT FEAR (which should be their slogan rather than A Better Deal). Put out the numbers, compare the costs, all of them. They need to tell voters the full story – except they can’t and won’t because they one wing of the War and Money Party. That fact is the reason UniCare won’t pass, “never ever” as Hillary once said, not that it’s not useful in other ways to the Dems.
Since the campaign for this legislation will be a get-out-the-vote ploy for Democrats, and we already know how Sanders can fold like a cheap tent at the last minute for the Democrats, it’s still going to require strong, relentless public demand to make the Democrats do the right thing for the people rather than corporate interests.
That’s going to take all of us stoking a hot, raging fire to hold their feet to.
> we already know how Sanders can fold like a cheap tent at the last minute for the Democrats,
“We” don’t “know” that. For example, Sanders extracted $10 billion for Community Health Centers, covering 20 million people, as the price of his vote for the ACA. If that’s your operational definition of “folding,” you’re setting a high bar.
I was referring to Bernie’s surrender before the convention after committing/promising/pledging over and over to take his campaign “all the way to the convention”. Donations kept coming in because, despite the odds, he was going to go the distance. That kind of commitment deserved support.
I think it was a disgrace to let all those young delegates down who needed to raise thousands of dollars on their own just to get to the convention, only to end up sitting there twiddling their thumbs and having their signs confiscated. Can you imagine the letdown, the feeling of betrayal?
To be clear, I said that Bernie ‘can’ fold like a cheap tent, not that he always does, but that was a big fold that many of us won’t soon forget. If he can do it once under the right pressure, he can do it again. After all, the Clinton Democrats still have some kind of ‘leverage’ (per Wikileaks), and Hillary is definitely on the warpath against Bernie.
Donations had slowed to a trickle at that point, he had almost no money by the time of the CA primary. I think it was legitimate for him to say he was taking it to the convention in order to pile as much pressure on to Clinton to see if she would give him any concessions. She did, over free college for more people and more funding for community health clinics.
In flight school we had an expression: “Flying successfully, and safely, requires a series of small corrections.”
All pilots know that to reach a destination successfully they (or, the auto-pilot) must constantly make small adjustments to air speed, altitude, direction, etc. When analyzing the veracity of a politician’s statment (promise) I don’t see any reason for not extending the same, inherently reasonable, understanding that “small corrections” might, not be only possible, but, inevitable.
In judging politicians I only look for purity of intention, not, necessarilly, in execution. I understand, and, appreciate your wariness. But, no one can predict the twists, turns, and, obstacles a movement will naturally experience. And, speaking for myself only, Bernie, and the current inertia of his health care proposal, represents the best chance yet that this enigmatic, national embarrassment of a problem can move forward successfully.
Regardless of Bernie’s motivations, I fear that it is a tactical mistake to introduce a bill that has no chance in hell of passing. It will serve to provide a fig-leaf for the carpetbagging Democrats (“we tried to pass single payer, but you saw that the Republicans blocked us!”) and essentially serve to sheep-dog the voters into the corp-Dem tent. The time to reform is when you have the political and legislative wind behind you… and when you have to have the right leadership in place to take advantage of that.
The optimists seem to have forgotten recent history — Obama in 2008 and Sanders in 2016.
“From the table, we can see that only one Senator — Tammy Baldwin — is putting her “Leans Democrat” seat at risk by endorsing BernieCare;”
I’m not getting why a democratic senator is putting her seat at risk by being for BernieCare? Are most democrats unalterably opposed to medicare for all? (unless one means that the 1% won’t fund her campaign or will use party shenanigans to prevent her re-nomination)
http://www.pewresearch.org/fact-tank/2017/06/23/public-support-for-single-payer-health-coverage-grows-driven-by-democrats/
Looking at some other polls as well, like a lot of issues it depends on the phrasing of the polling question, but I wouldn’t say that being for medicare for all is particularly hurtful to a candidate, especially a democratic candidate….
AND this
http://thehill.com/policy/healthcare/339247-poll-support-grows-for-single-payer-healthcare
“60 percent of Americans who were surveyed said the federal government is responsible for providing healthcare coverage to all Americans, compared to 39 percent who said it was not the government’s job.”
Tammy Baldwin is both an excellent politician (faint praise) and a longtime single-payer supporter (at least verbally). But she went big for HRC. I think, and I think she thinks, that her political prospects would be worse if she were not on this bill.
The optimism of this analysis is breathtaking in the light of American history.
Just for starters:
That the State as presently configured and controlled can somehow be made to work for the benefit of the average American in the particular area of healthcare.
A failure to grasp that social-democratic traditions have never been much more than a fringe movement in American history. The one exception being the New Deal.
A failure to consider that creating a space for seriously taking on all dimensions of economic inequality (including healthcare) will probably have to come from creative thinking within the Jeffersonian tradition not the social-democratic tradition.
Sanders’s agenda polls well; and he polled well himself in the primaries especially with independents. That doesn’t reflect an American political tradition? Of course it does.
The New Deal grew out of the Great Depression; and now the Great Recession has recruited people to supporting left-wing policies too.
Yes, I am fundamentally optimistic, despite my pose of light irony.
So were the abolitionists, and there is no more slavery.
After 7 years of railing at the ACA, the GOP leadership is standing in the middle of Main Street naked. Their constituents are beginning to realize that there isn’t an easy solution, but they have definitely figured out that healthcare insurance coverage is a good thing.
It is unclear at what point most Americans figure out that the propaganda against the ACA and these types of initiatives are fake news. I think Americans are starting to realize that their insurance companies have the types of “death panels” that only socialized medicine is supposed to have.
> the GOP leadership is standing in the middle of Main Street naked
As will, quite shortly, Pelosi, Schumer, McCaskill, etc.
It’s funny you should mention this. I actually think democratic republicanism and social democracy are compatible. Perhaps we might see social democracy as the economic expression of a democratic republicanism that never quite made it intact into the economic sphere.
In terms of how optimistic to be, I don’t know. But if you start out defeated, you stay defeated.
We’re not sure what DiFi is going to do. Apparently Adam Schiff has been attending fundraisers for him for Senator.
I think it’s great that Bernie gets this out there and drags the conversation where we want it. Just because it won’t pass this year or next, it allows for further educating the population of what they could – and should – have. Bernie is using his time while the Dems are in the minority very creatively and I like that.
Matt Taibbi is optimistic:
Single-Payer Movement Shows: Life After Trump May Not Suck
http://www.rollingstone.com/politics/features/taibbi-single-payer-effort-shows-life-post-trump-may-not-suck-w503498
I think, ultimately, it’s a wedge issue, and all this bill does is place the wedge at the place where the party will split. Soon, the DiFis of this world won’t matter nearly so much.
perspicacious!
(had to check to make sure of the meaning of the word that came to mind–yup!)
discerning, shrewd, perceptive, astute, penetrating, observant, percipient, sharp-witted, sharp, smart, alert, clear-sighted, farsighted, acute, clever, canny, intelligent, insightful, wise, sage, sensitive, intuitive, understanding, aware, discriminating
I think you are correct. And I think it shows Sanders 16 campaign has legs because the message resonates.
Whitehouse, Schatz, Udall and Merkeley are a posse. Buddies. Self-important halfwits, usually. Interesting to me that they saw Sanders bill as the place to go. Largely a form of preening and an appeal to Sanders faction, but maybe a wariness toward Obamacare. All guesswork. I have no knowledge of actual chatter and decisionmaking. But this group has long been keen on the idea that they are the rising class of leaders.
Booker is odd duck. May be afraid of challenge from Bernie faction. May, wildly, think he has a chance to be President.
Gillibrand, Harris, Franken are all Bluedogs trying to hide stripes in hopes ofcattracting Bernie votes in 2020 primaries.
Warren is a bit more sincere, with the same motive.
Hirono is sincere, I think. With limited knowledge, I have always liked her.
Missing Sherrod Brown is no surprise to me. That he ever gets any good reviews fromm Left is travesty. He is Bluedog hack, and nasty person.
In short, we are not seeing leaders. We are seeing pols fishing for votes where they think fish may be biting.
As a Minnesotan, I have to defend Al Franken. He was pro-universal healthcare back when he ran for the first time in 2008. I think it’s unfair to paint him with the same brush as other opportunists that recently jumped on the Medicare for All bandwagon.
I do acknowledge though, and was very disappointed, that Franken was gung-ho for Hillary in 2016.
my thoughts too…Lambert
@Livius: In my living area, suburban NYC, I really do not see how physicians can employ the “this bill will put me out of business” argrument as individual practioners no longer exist. Physicians are employed by large corporations. When 75% of your fellow waiting room occupants are clearly on Medicare or Medicaid that any attempt to broach the “government will drive us out of business” will inspire peals of laughter.
Maybe they can go back to being individual practitioners with M4A.
Thank you for this, Lambert. As a Granite Stater, I was pleasantly surprised, nay, gobsmacked to see Jean Shaheen among the co-sponsors. With few notable exceptions (her regrettable about face on fast track among them), she strikes me as someone who has made it her life’s mission to avoid any interesting stances in politics.
Also, the New Hampshire primary.
If you are referring to 2016, Bernie’s landslide win does not appear to have made much of an impression on Annie Kuster or Carol Shea Porter, who have yet to support HR676. I don’t see Shaheen running for a third term in 2020. Maybe that’s why she, and not the rest of our all female! all democrat! delegation is cosponsoring; testing the waters as it were. Not that I’m cynical.
I was less precise in my thinking; it simply appeared to me that MedicareForAll would be on the table in the primary; whether or not Shaheen won, she’s surely a powerful member of the Democrat establishment, so it will play a role in NH 2020.
This bill will have a devastating effect on the jobs of the 2.5 million people who work in the health insurance business. (source: https://www.statista.com/statistics/194233/aggregate-number-of-insurance-employees-in-the-us/) It would be politically wise for proponents of single payer to have a credible, well-funded program, along the lines of past proposals for dealing with job losses from cutting back the defence budget, to help these workers find new jobs.
Per your link that’s the number for the entire insurance industry. A link from the text puts US “home-office health insurance employees” at 525,600 as of 2015. See my comment above re attrition rates, possible H1B workers, etc.
Yes and what of the investors in those companies?
I don’t know about yall, but said investors are pretty far down my list of things to worry about in this discussion.
Perhaps Moloch will take care of his own.
Perhaps UBI, or a Jobs Guarantee? See oaf and JonA below.
No one defended workers when the passage of NAFTA led to the loss of nearly one million jobs. So why do these people deserve special treatment?
They don’t, but since involuntary unemployment exists and rank and file insurance employees don’t have much choice, failure to deal with this hurts the bill’s chance of passage one day. They provide a convenient excuse for Democrats in Congress not to vote in favour and to pretend that private insurance companies have some kind of valuable role.
One reason to do something about them is to eliminate another source of opposition.
And the true question of it is thus:
How many of those workers hate their jobs and long to do something else yet stay because they GET health benefits?
I humbly suggest tens of thousands in the industry and hundreds of thousands of others, employed but similarly stuck for benefits tied to private insurance thru their crappy jobs would be happy to use a real safety net to pursue other opportunities.
People may surprise when allowed to dream without fear.
Yes, it might be offset by those with enough money to retire but only working for health benefits (this admittedly is a small percentage of people, most people will not have enough money to retire before 65, most people need to wage slave up to 65 and Beyond, health insurance or not, but maybe it’s still enough to open up some new jobs for people).
A lot of those “2.5 million people,” including several family members, are employed in the precariat positions you are concerned about. With consolidations and m&a’s and outsourcing and “more and more work from fewer and fewer people for less and less pay,” they never know when they will be gobsmacked with a “layoff” or opportunity to train their Mumbai replacement. I know of planned layoffs/firings that were scheduled for just before Christmas but the optics just got so bad in light of the recent hurricanes (“Work extra hard to keep us profiting in the crisis, now you’re fired”) that the actions have been put off for a month or so.
You really think that people at the slave labor gig-job precariat level of the medical UNsurance Industry will be so very invested in their “jawbs” when they will get the concrete material benefit of actual health care, and a chance to move over into actually doing some good in the administration of the universal program?
2.5M is for the entire insurance industry, not health insurance – see comment
yes if they get a chance to move over to another job, just like anyone who loses their job, but if they don’t medical insurance doesn’t pay the rent … but most everyone has been unemployed once or twice or several times in their life (this is the modern economy duh), so one adjusts and hopes and looks for work.
The government would certainly have to do some serious hiring to staff up for nationwide single-payer. With sufficient de-programming away from the profit motive, wouldn’t at least some of the current workforce in private insurance be valuable to running Medicare for All? They can’t all be irredeemable.
We could also borrow the private sector idea of buying out final work years and/or pensions. We could offer lump sums based on average incomes by age. Maybe couple that with larger amounts and longer timeframes for unemployment benefits, new educational pursuits, and/or paid-for training, and the runway to new career options starts to look a lot smoother.
Unemployed could move over to the hospitality/travel sector. That’s where I’m planning on spending the money from my left pocket!
That it takes 2.5 million people just to manage our system of paying for healthcare, shows how desperately we need single payer. I can’t possible think of a greater waste of humanity then paying so many people to control costs when the final result is so over priced.
So, when blue collar workers lose their jobs, that’s just market forces at work. But when white collar workers lose their jobs … . I have little sympathy for an industry which charges too much to do too little paperwork, plus has a track record of gaming the system so egregious. Sure, people will lose their jobs, let them apply to Medicare to do the work needed for all of the newly covered. Of course, far fewer will be needed.
There will still be work for insurance companies. I am on Medicare and have a “Medicare” supplement plan (BC-BS) to cover much of what Medicare does not. There will be people, still who do not want anything less than the very best care and they will need their Cadillac plans, too.
Bernie rocks! This is long overdue. Why not throw in a *liveable* UBI while we’re at it?
Be nice to use UBI as unemployment insurance for an interim before a job guarantee.
With apologies to the Phreak Brothers:
>critical medical care will keep you alive
through periods of no income
better than income will keep you alive
through periods of no critical medical care
yes you’ll be alive you’ll just be homeless! True it’s not dead but noone actually wants to become homeless, in fact it’s a huge fear people have, fear of losing work and becoming homeless. Get real if you think only health care matters and not income (at least for those living paycheck to paycheck). And some demographics like young people being mostly young and healthy have a lot more to fear from losing shelter and other economic hardships than from loss of healthcare. So yea people’s incomes matter to them almost like life and death. But it could be offset.
Because a Jobs Guarantee is more politically feasible and better policy (though a UBI might supplement a JG).
So here is an issue I haven’t heard about much. What happens to all the investors in those insurance health care companies that go out of business or lose most of the market value, or the thousands of employees that no longer have a job? Does it matter and what do you do about it?
We still have insurance companies here in Canada. You can buy this privately, but more often it is an employee benefit. They cover such things as income replacement, life insurance (of course), prescriptions, ophthalmologists and eyeglasses and dental, which are not covered by most provincial Health plans. They also will insure for non-‘standard’ medical treatments such as naturopaths, massage not prescribed as physiotherapy, and such. I remember several going broke back in the ’90’s but the word then was the problem was bad investments.
We also have to buy insurance for non-health-related stuff — auto, home, business, and of course, credit default swaps. They can still make lots of money!
This is a net positive to remove those in the re-insurance industry from their jobs. Medical insurance extracts more than 17% from National GDP. Who wouldn’t want to take an axe to that?
Also, I thought that investors were entitled to earning dividends and stuff by virtue of taking risks? Well, maybe sometimes they lose.
I think, too, of homeowners who lost their homes, so maybe there could be something like HAMP to make whole the insurance investors? Yes, that was snark.
I said above on employees, to eliminate another source of opposition, and if money is at stake it will be very loud.
approx. 325 million americans, roughly 235 million of which are voting age. As marym points out the entire insurance industry is +/- 1% of that number so if they will be loud as you claim, they will be talking with their wallets, and as others have pointed out, of those 2.5 million insurance employees, most are likely in the precariat so will not be the funders of this projected noise, and will benefit from medicare for all, and the one’s of those who are reaping the massive profits from their protected position in the PPACA (hahahahathat’s funny patient protection, should be patent protection at the least, or payola protection) I have zero sympathy and hope they go broke and have to find a place in one of the ubiquitous tent cities sprawling across our great land…Millions upon millions of americans lives have been ruined by these people. There’s a commonly used acronym, the FIRE sector, it stands for Finance,INSURANCE, and Real Estate. Their bloated by theft of hope massive rentier balance sheets which back all variety of securitizations and derivations are a scourge on the planet.. These are the people whose jobs you’re worried about? Why?
and not to pile on too much, but lambert likes to refer to concrete material benefits, one of which would certainly be medicare for all, and may very likely induce the non-participating voters (54.9% of eligible voters voted in the past election, as per wikihttps://en.wikipedia.org/wiki/Voter_turnout_in_the_United_States_presidential_elections) to come out and vote, because we know who’s screwing us over…it’s the people whose severance pay you’re worried about (severance pay? what’s that? I’ve had owners of pharma patents stiff me and say “what are you going to do about it?” I’m a construction worker so the answer to that question is, other than never working for that person again ((“…but I would give you references!”…fool me once and all)) nothing at all) I say they made their bed and hopefully will have to sleep in it.
Does it matter? Yes. But, those investors should have thought about that and recognized the risk. We are an ownership society, and they will need to own their fate without complaint. Which brings me to the poor employees, outside of the C-suites, of AHIP companies (not all insurance company employees, by a long shot). “Links” today had a piece from the NY Post, of all places, about “the day the working class died,” 40 years ago this week when Youngstown Sheet & Tube closed and sent 5,000 workers home. As a then 21-year-old “graduate” of the working class, this deeply affected me as the first major tremor of an earthquake that lasted, well, forever. Suffice it to say that from the late-1970s until now, I have heard no (OK, very few) wails or gnashing teeth from the white collar world of work when steelworkers, tool & die makers, machinists, textile workers, autoworkers, chemical workers, and longshoremen, who were the backbone of a USA that could make things, and did, had their worlds destroyed by the neoliberal consensus.
I’ve told my mostly academic colleagues in medicine and the basic medical sciences that they/we are on the menu, too. Ask a diagnostic radiologist who competes with an Indian radiologist who works while he sleeps, reading high-resolution images available with the click of a mouse, for pennies on his dollar. Anyway, these AHIP employees should be taken care of, and I expect they will be. While my empathy feels their fear, my sympathy lags. Let them “re-train” if that’s what it takes, just like the subjects of Amy Goldstein’s recent book, Janesville: An American Story. Or find work in their local Medicare-for-All office, where their skills are surely transferable? This is a problem that cannot be solved under the neoliberal dispensation, but that doesn’t mean it is unsolvable.
Diagnostic radiologists’ jobs aren’t quite on the line. A Hospital is liable for any reads that is inaccurate. It might sound easy when you are asking a radiologist to read an Xray/CT Scan/MRI when it is for something you are looking for, but what if the case is:
“Scan is for determining if surgical instruments are within patient” and turns out it wasn’t an instrument, it was a sponge?
The hospital is liable already, any further misread compounds the liability problem. Despite the talk of “outsourcing” medical diagnostics, due to the highly liable nature of our current HealthCare climate it is HIGHLY UNLIKELY. So that radiologist’s job is fine.
> What happens to all the investors in those insurance health care companies
They’d better head for the exits now!
“What happens to all the investors in those insurance health care companies” “Hopefully they lose a $hit ton of money. Just kidding, kinda. I think most health insurance companies have had decades to skim ever larger moneys from the rest of us. The initial investments have probably long been recouped. Anyone buying stock later on was just speculating. When you speculate on the future of a shockingly wasteful industry, you can’t expect to win forever. As for the workers, other then prison guard or maybe drone pilot, I can’t think of a more soul crushing and wasteful way to employ people.
(“BernieCare,” as I suppose we must call it)
I think we can come up with a better name than that. BernCare? BernTreatment? Bernthehealthinsuranceindustrytotheground?
…latter would be perspicacious…
Identity politics are already being used to attack BernieCare (I vote we adopt it out of the gate instead of letting the corporate shills turn it into a sneer). There’s a meme going around on social media with a pic of Rep. Conyers complaining that he’s been proposing his bill since 2003 and now Bernie is getting all the credit for single-payer. It’s clear what the intent is because I’ve already been attacked for pointing out having a separate proposal in both Houses of Congress is SOP, and that some progressive Democrats have issues with his bill for reasons mentioned by several commenters here.
It appears, then, that the opposition is going to once again paint Bernie as a privileged white guy shoving aside the dedicated African American to get all the glory.
Conyers’ statement:
>“I applaud Senator Bernie Sanders’ introduction of the Senate companion to my Medicare for All bill and all of the momentum he has garnered in support of a universal single-payer healthcare system…”
>source: https://conyers.house.gov/media-center/press-releases/conyers-applauds-bernie-sanders-senate-introduction-medicare-all
comparison of house and senate medicare for all bills
http://healthoverprofit.org/comparison-chart/
That is the link I included in the next post, thank you.
Hello? Paying for this may be complicated but it is not difficult. We are already paying twice as much for comparable service as other advanced nations:
Per capita spending health care 2015
United States: $9451
Canada: $4608
France: $4407
Japan: $4150
United Kingdom: $4003
Miraculous Finland: $3984
Of course, when we look at such a list we see the savings that could be achieved. The plutocrats see, instead, the lost profits were we to undertake a national healthcare system.
As those who understand Monetary Sovereignty know, Medicare for All needs no “funding mechanism.”
What is the “funding mechanism” for the military? What is the “funding mechanism” for the Supreme Court? What is the “funding mechanism” for the White House?
What is the “funding mechanism” for the NSA, the CIA, FEMA, the FBI, and every one of the thousands of federal agencies? In a Monetarily Sovereign government, the money doesn’t “come from” anywhere.
Dollars are is created, ad hoc, every time the federal government pays a creditor. Federal taxes do not fund federal spending.
In fact, the discussion of a “funding mechanism” is a device to prevent Medicare for All. The fake need for a special tax or for a “trust fund,” are lies about a program some in Congress wish to prevent.
Bottom line: The federal government could eliminate FICA and easily provide Medicare to every man, woman, and child in America. No “funding mechanism” wanted.
We may understand this
But it’s counter intuitive and if General understanding is a prerequisite to M4A it’s doomed
Got to make “financing” arguments that are comprehensible. Probably best to focus on savings, net…
Those who lie because the truth is “inconvenient” or “hard to understand,” repeatedly will find their position undercut by facts slipping out, until nothing they say is believed.
Better to tell the truth and defend it with facts, than to tell a lie and continually search for new lies to defend it.
The only absolute defense for Medicare for All is the fact that it costs taxpayers nothing and is a benefit to everyone.
Bernie’s Bill makes a good case for single-payer which is much more comprehensive than Canada’s healthcare system. As for paying for universal health care, in Canada about 30 % is paid through the private sector, e.g. prescription drugs, dentistry and optometry and about 70% is paid for by various levels of government. The Federal Government establishes guidelines in order to make delivery in poor provinces equivalent to those in richer provinces. This past year, the Minister of Health offered each province money to establish home care and mental health care services. The only criteria was that the money must be used for those two services and all the provinces finally agreed to accept the terms (which, in my view, were reasonable).
There is a constant and on-going push to privatize our healthcare and/or to charge fees for service. We sometimes have options, e.g., to pay for blood tests or wait to be served by the system. The Federal Government administers healthcare to the military and veterans, and for prisons and for some services for the RCMP which cover drugs, dental and some optometry services. Other citizens can get private (e.g. Blue Cross) insurance for those needs.
Sometimes our government (the Conservatives under Harper) tries to undermine our system from within by reducing Federal monies for health. Over time, the proportion of Federal dollars spent on healthcare has gone down.
Bravo, Bernie!
As for insurance companies not having work to do after the US gets single-payer, rest assured, that they are very inventive. There are all kinds of insurance companies promoting various health schemes in Canada. For example, our pension system is called CPP (Canadian Pension Plan) and one insurance company uses that same acronym to promote health insurance above and beyond what is now provided in our single-payer system. Insurance companies are very inventive (not!) and will create needs that aren’t really there, believe me!
Good topic. Good discussion. Lots to be hopeful for.
And let’s not forget in addition to Health Care it includes Dental and Vision.
I like to count things and, since dental is a most obvious health issue,have been counting ” bad mouths” in sets of ten continuous encounters for about a year now. Many more folks need dental work–by visual observation–than I ever thought.
And let’s not be so fast to discount those employed Health Insurance Professionals so fast–the few I know have very candid inside observations
on medical cost drivers and fixes that would benefit a MfA system.
Not surprised to learn that our cowardly Senator Ben Cardin hasn’t endorsed this bill, even though he’s in a safe seat in a blue state [Maryland]. Time for some “communication.”