Yves here. This discussion of the widespread misapplication of an early study on the risk of opioid addiction illustrates why scientific studies are met with much more skepticism than in the past. And this was before the era of big money distorting research.
By run75441. Originally published at Angry Bear
Some History
In 1980, a letter to the editor of the New England Journal of Medicine by the Boston Collaborative Drug Surveillance Program stated “the risk of addiction was low when opioids such as oxycodone were prescribed for chronic pain.” It was a brief statement by the doctors conducting the study which was cited many times afterwards as justification for the use of oxycodone.
In a June 1, 2017 letter to the NEJM editor, the authors reported on the broad and undocumented assumptions made as a result of the 1980 Letter on the Risk of Opioid Addiction.Using bibliometric analysis of the impact of this letter to the editor, the citations of the 1980 letter were reviewed to determine the citation’s portrayal of the letter’s conclusions.
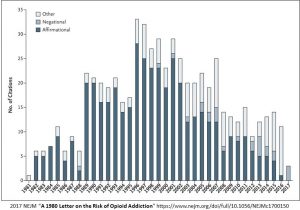 Identified in the bar chart are the number (608) of citations of the 1980 letter over a period of time from 1981 to 2017.
Identified in the bar chart are the number (608) of citations of the 1980 letter over a period of time from 1981 to 2017.
“72.2% (439) cited the letter as evidence addiction was rare in patients when treated with opioids such as oxycodone. 80.8% (491) of the citations failed to note the patients described in the letter were hospitalized at the time they received the prescription.”
There was a sizable increase of citations after the introduction of OxyContin (extended release oxycodone) in 1995. As the analysis noted “affirmational citations of the letter have become less common in recent years in contrast to the 439 (72.2%) positive and supporting citations of the 1980 correspondence in earlier years. The frequency of citation of this 1980 letter stands out as being unusual when compared to other published and cited letters. Eleven other published, stand-alone, and more recent letters on different topics published by the NEJM were cited at a median statistic of 11 times each.
Citations of the 1980 stand alone letter on “addiction being rare” from the use of opioids such as oxycodone failed to mention, the patients administered to were in a hospital setting as noted in the letter by Porter and Jick. Overlooked, a mistake by the people citing this letter? “In 2007, the manufacturer of OxyContin and three senior executivesof Purdue Pharma plead guilty to federal criminal charges that they misled regulators, doctors, and patients about the risk of addiction associated with OxyContin.”
![]() Organization: “An early manifestation of the opioid abuse, addiction, and overdose problem occurred largely in the rural regions of Kentucky and other parts of Appalachia after the introduction of Oxycontin. A brand name for oxycodone, OxyContin was introduced in 1996 by Purdue Pharma and aggressively sold to doctors. Sold as a less-addictive alternative to other painkillers as it was made in a time-release formulation, allowing for a slow onset of the drug, and not a hit all at once which is more likely to lead to abuse. When used as prescribed, Oxycontin was safe. When ground up, it’s slow release characteristics were marginalized.
Organization: “An early manifestation of the opioid abuse, addiction, and overdose problem occurred largely in the rural regions of Kentucky and other parts of Appalachia after the introduction of Oxycontin. A brand name for oxycodone, OxyContin was introduced in 1996 by Purdue Pharma and aggressively sold to doctors. Sold as a less-addictive alternative to other painkillers as it was made in a time-release formulation, allowing for a slow onset of the drug, and not a hit all at once which is more likely to lead to abuse. When used as prescribed, Oxycontin was safe. When ground up, it’s slow release characteristics were marginalized.
The aggressive sales pitch led to a spike in prescriptions for OxyContin of which many were for things not requiring a strong painkiller. In 1998, an OxyContin marketing video called “I Got My Life Back,” targeted doctors. In the promotional, a doctor explains opioid painkillers such as OxyContin as being the best pain medicine available, have few if any side effects, and less than 1% of people using them become addicted.
Shortly after 1996, Porter and Jick’s letter citations doubled and continued to be cited in a positive fashion with few negative citations and a failure to mention the hospital setting where the drugs were administered.
More Recently
By 2015 over a six-year period, more than 183,000 deaths from prescription opioids were reported in the United States. Today, millions of Americans are now addicted to opioids.” In part much of this was the result of doctors being told there was a low risk to opioid addiction.
Figure 2 shows each year being progressively worse and reaching a record high of 71,568 deaths (2017) in the US due to all drug overdoses as reported by the Centers for Disease Control (CDC) in their “Provisional* estimates on U.S. drug overdose. According to the CDC this is a record and represents a 6.6% national increase in overdose deaths over 2016.
At the end of the 12-month period of January 2018, the reported deaths was 69,703. The final and predicted number of deaths is expected to be as high as 71,568. 0.18 of 1% of the reports are pending the completion of investigation (numeric within chart). *Underreported due to incomplete data.
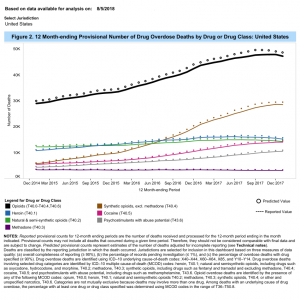 *Provisional counts of all drug overdose deaths are underestimated relative to final counts. The degree of underestimation is determined primarily by the percentage of records with the manner of death reported as “pending investigation” and tends to vary by reporting jurisdiction, year, and month of death. Specifically, the number of drug overdose deaths will be underestimated to a larger extent in jurisdictions with higher percentages of records reported as “pending investigation,” and this percentage tends to be higher in more recent months”.
*Provisional counts of all drug overdose deaths are underestimated relative to final counts. The degree of underestimation is determined primarily by the percentage of records with the manner of death reported as “pending investigation” and tends to vary by reporting jurisdiction, year, and month of death. Specifically, the number of drug overdose deaths will be underestimated to a larger extent in jurisdictions with higher percentages of records reported as “pending investigation,” and this percentage tends to be higher in more recent months”.
In 2018 law makers questioned Miami-Luken and H.D. Smith wanting to know why millions of hydrocodone and oxycodone pills were sent (2006 to 2016) to five pharmacies in four tiny West Virginia towns having a total population of about 22,000. Ten million pills were shipped to two small pharmacies in Williamson, West Virginia. The number of deaths increased along with the company and wholesaler profits.
For context, the nearly 72,000 drug overdose deaths (spurred by the ongoing opioid painkiller addiction epidemic, including the increased use of more potent synthetic opioids [fentanyl]) outpaced fatalities from suicide, or from influenza and pneumonia, which claimed about 44,000 and 57,000 lives in 2016. It nearly rivaled the approximately 79,500 people who die from diabetes-related complications each year in the U.S. (the 7th leading cause of death).
Nearly 150,000 Americans die each year from accidents such as car crashes, injuries, or accidental overdoses. If the CDC’s latest figures are accurate, drug overdoses could account for nearly half of accidental deaths.
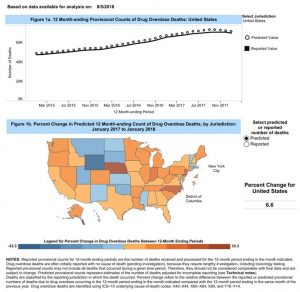 As tends to happen with public health epidemics, overdoses have an outsize effect in certain regions. For instance, the biggest spike in fatalities by percentage occurred in Nebraska, North Carolina, New Jersey, Indiana, and West Virginia (33.3%, 22.5%, 21.1%, 15.1%, and 11.2% rises, respectively). But areas like Wyoming, Utah, and Oklahoma experienced declines of 9.2% to 33%.
As tends to happen with public health epidemics, overdoses have an outsize effect in certain regions. For instance, the biggest spike in fatalities by percentage occurred in Nebraska, North Carolina, New Jersey, Indiana, and West Virginia (33.3%, 22.5%, 21.1%, 15.1%, and 11.2% rises, respectively). But areas like Wyoming, Utah, and Oklahoma experienced declines of 9.2% to 33%.
With the clamp down on opioid prescriptions by doctors due to the abuse, addiction, and overdoses, those addicted to opioids turned elsewhere. Again Recall Report;
In 2015 heroin overdose deaths in the U.S. surpassed the number of deaths by gun homicide for the first time ever. In addiction treatment facilities around the country, heroin addiction is becoming the most common reason to enter treatment, surpassing even alcohol addiction.
In combatting the prescription painkiller addiction epidemic, public officials may have unwittingly contributed to the heroin epidemic. As prescription opioids became more difficult to obtain and more expensive, addicts turned to a cheaper similar high: “heroin.” Mexican drug cartels were more than willing to supply the demand and much of the cheap heroin in use in the country now comes through Mexico.
The ease of accidentally overdosing can have a tragic consequence resulting from the abuse of opioids and heroin as they act upon areas of the brain controlling breathing by depressing it. Too much of an opioid drug can result in a person stopping breathing and their death. Add alcohol or a sedative and the risk increases. The advent of Narcon in an injection or a nasal spray format is an antagonist to the effects of opioids and heroin heroically reversing the effect of an overdose.
Stopping the abuse of opioids is an important measure in gaining control of the growing number of people becoming addicted to opioids and dying from its abuse. Once addicted, in many cases treatment is essential with detox and withdrawal the first painful step back to a normal life. Without supervised treatment and/or residing in a residential treatment center, the return to opioid usage and addiction is easy as the cravings for using it again are powerful. As a resident in a treatment center, therapy, support, and medical treatment with drugs is possible. The abuse of opioids and addiction will remain a problem for years to come until the supply of it is brought under control.
Prescription Painkiller Addiction: A Gateway to Heroin Addiction, Recall Report Organization
A 1980 Letter on the Risk of Opioid Addiction, NEJM, June 1, 2017
Supplementary AppendixNEJM, June 1, 2017; Copy of Porter and Jick’s letter to NEJM in 1980.
Provisional Drug Overdose Death CountsCDC, National Center for Health Statistics, August 5, 2018


This is a case of the pendulum swinging way too far with potential dire consequences for health. According to a recent CDC study, linked below, the number of number of deaths from prescription opiates has been over-estimated. And there are HUGE health dangers associated with drastically curtailing the freedom of physicians to prescribe opiates or drug companies from manufacturing this medication.
A new CDC study gives an estimate of 17,087 deaths a year due to prescription opiate overdose. That’s a horribly large number, but it’s half the previous figures that were floated and is small compared with the number of deaths per year from alcohol, which no one is considering outlawing.
But the more important issue is that the alternative, but far less effective painkillers are the NSAIDS, i.e., aspirin and ibuprofen, and they themselves are very dangerous. They have long been known to damage kidneys, and recent studies have shown that they cause heart attacks and strokes. There don’t seem to be good authoritative estimates for yearly deaths attributable to NSAIDS, but it could well end up rivaling that of prescription opiates.
And this doesn’t count the number of deaths per year from inadequate pain medication, either from suicide due to intractable pain or from heart attacks and stroke due to the extreme stress.
I’ll give you my own example. I was a completely healthy 60 year old with lifelong normal lab results. I woke up one morning in excruciating pain from a torn rotator cuff. The pain was unbearable. Knowing that my physician was terrified of prescribing opiates, I started taking ibuprofen. The ibuprofen barely alleviated the pain, but it was better than nothing. Shortly thereafter, I developed shortness of breath, and it turned out that I was extremely anemic. My lab results showed an alarming creatinin level of 1.9 -i.e., my kidneys were shot. Eventually, my kidney function improved, but it never went back to normal.
What makes this push to drastically curtail the use of prescription narcotics all the more irrational is the shakiness of the assumption that people wouldn’t become addicted to opiates if doctors didn’t prescribe them. That might be true in some cases, but I suspect it’s a minority of cases, and I suspect that those are the people could most successfully overcome the addiction. But people don’t need physicians prescriptions to become addicted to cocaine and meth and I suspect that they don’t need doctors’ prescriptions to find their way to street opiates either.
Here is a good summary of the recent CDC estimates of prescription opiate deaths:
Thanks, R. Greenberg. I don’t have any need for opiates but seeing how the pendulum has swung way too far in a restrictive direction, I am now terrified about getting proper pain treatment should the need ever arise which none of us can be sure it won’t. I’ve even heard discussion of having “opiate-free ERs” which as you note is a horrible idea.
Thanks for this comment. My mother, who doesn’t tolerate oral narcotics well and is in excruciating pain from arthritis, stenosis, and sciatica (she turns 89 this month), has a PCP who refuses to increase the fentanyl patch (which she can tolerate) beyond 50mg to a therapeutic dose (probably around 75 per the ortho who still gives her cortisone injections (that at this point only provide relief for a few weeks although Medicare doesn’t allow them now often than quarterly) and first initiated methadone at a starting dose of 12).
About a month ago she became short of breath and dizzy even after taking the very few steps her pain allows her to take (maybe a car length). Sure enough, the NSAIDS that provided her some relief had eaten a hole in her stomach and she was bleeding internally.
She had to go to the hospital for a transfusion. This is a woman who has only ever been hospitalized to give birth! When I accompanied her to the endoscopy she told the anaesthesiologist who was asking whether she wanted to suspend her DNR/DNI for the procedure, she exclaimed, “NO! With this arthritis pain my life is miserable!”
(Later she commented to me that she thought it somewhat underhanded for them to ask that question at such a vulnerable time as thus people who had carefully thought through their wishes might in the moment make a choice that was in fact not what they really wanted.)
Now she has been switched to Celebrex which is gentler but she cannot take enough to really help with the pain. It just kills me that her PCP, whom she unfortunately adores, is permitted d/t ignorance about fentanyl to maximize my Mom’s suffering.
*more often than quarterly
*endoscopy last week
Boy, do I miss that edit function! Was also going to ask for the link.
Your mother sounds like me. I have been taking opioids for years and am now to the point where they don’t work unless I double or triple the dose. Because of this fear about opioid addiction, I cannot get my doctor to change either the number of pills or the dosage. Nor can I take any over-the-counter NSAIDS because I have kidney problems too. Plus, my Medicare insurance company refuses to pay for Lidocaine patches. The pharmacist told me they cost $300 for a box of 10 patches and that desperate people who have to buy them just cut them into smaller pieces to make them last longer. I used to take Celebrex, but it was taken of the market because of serious side effects. Are you telling me it’s back again? There are no good choices and getting old sucks.
Celebrex IS back. Yikes, need to look into it having been taken off the market.
Yup, my Mom buys Lidocaine patches and cuts them up. Anyway she pays for all her meds out of pocket cuz she thought when W passed part D it was an immoral transfer of wealth from the young to the old and big Pharma. She had no idea she would live to be this old since mostly her family makes it into their late 70s.
I also got her a whole plant pain relief topical cream from CA–Dr. Kerklaan, equal parts THC & CBD. And spending some time in zero gravity seems to help. Using a combination of things, some days are less awful than others.
I am sorry you are going through the same thing.
Please join the fight
Don’t Punish Pain Rally
C-50 Coalition of State Pain Advocacy Groups
Your presentation is in bad faith and intellectually dishonest.
You are presumably citing the August 31, 2018 CDC study. It states that 40% of opiod death in 2016 were from “a prescription opioid”. That means the CDC confirms the opioid death levels that Nobel Prize winner Angus Deaton and his wife Ann Case have now confirmed twice, in 2015 and again in 2017. And had you bothered reading Case-Deaton, you would know their work was based on CDC data!
You are also incorrect that NSAIDs are less effective than opioids. For some types of pain, they are better. I have have excruciating pain several times in the last five years, and I have a very high pain tolerance level. I have always found high dose NSAIDs to be more effective that opioids. Mind you, I was still in a lot of pain, but the NSAIDs made a dent while the opioids didn’t and made me feel feel worse in other respects. Bizarrely, oral surgeons hand out Vicodin like candy when ibuprofen is the best pain killer for dental pain.
There is also evidence that opioids become less effective in treating long-term pain. And your claims regarding health risks of NSAIDs are wildly exaggerated. They represent a risk to kidneys only in patients who already have impaired kidneys. This is from the National Kidney Foundation:
https://www.kidney.org/atoz/content/painmeds_analgesics
Quite a different picture than the one you gave.
You likely had an undiagnosed kidney ailment before you took ibuprofen (I prefer aspirin and naproxen sodium, which is a chemical cousin to ibuprofen, but to each his own). The big risk, which you do not mention, is that of stomach bleeding and intestinal irritation. Opioids, by contrast, regularly produce constipation and nausea, in some cases so severe that the patient has to discontinue the med. See below for details:
https://www.ncbi.nlm.nih.gov/pubmed/18443635
According to this letter published in the JGIM the odds for opiate addiction are 3.4% after surgical intervention (hospitalization) and 7.2% after medical –out of hospital– prescription.
This is to clarify why is important to indicate if the opioid was prescribed at the hospital, and to indicate how deceptive was the “less than 1% addiction rate” propaganda.
Long-term analgesic use after low-risk surgery: a retrospective cohort study.
And here in Tucson, one of our big local hospitals is going after the traffickers, er, manufacturers and distributors. Link:
https://www.kgun9.com/news/local-news/tucson-medical-center-suing-opioid-manufacturers-distributors
I wish people would choose their words more carefully. In the blurb for this post the phrase used was ” for overly-casual prescription of these drugs.” This was not a case of over-casual prescription. This was a case of the drug manufacturer deliberately creating a false impression regarding the safety of their product in the minds of doctors. Those same manufacturers did more than look the other way to make sure an illicit pipeline supply of “Oxy” was also available.
When I lived in Florida my back went out: it’s a lifelong recurring problem. I gimped to a “back clinic.” The waiting room had what looked like a bunch of junkies. They didn’t take my insurance but it was visits were oddly affordable so I offered to pay; this didn’t strike them as odd at all.
Eventually I was called and a nurse asked what’s wrong and I told her “I lifted something too heavy now I’m having muscle spasms.” She smiled and asked what prescription I wanted. I asked her “don’t you want to look at my back?” She looked confused and I told her put her hands on what anybody could feel was a serious problem, a literal bundle of muscles and nerves. She said (I’ll never forget this) “oh – something really is wrong – I’ll get the doctor” like it’s atypical to have a verifiable problem.
It was then I realized I’d wandered into a pill mill. I left and found a real doctor who prescribed a limited number of muscle relaxant – just enough to break the cycle of muscle spasms – plus non-narcotics and physical therapy. Pharma companies, healthcare providers, and all the rest know exactly what they’re doing pushing this junk.
Aw, heck. I just did the same thing. Lifted something and then I twisted my back. Ouchy-ouchy, Slim is grouchy!
What has helped the most? A massage, that’s what!
No drugs for this camper. I don’t need ’em.
Epsom Salts (magnesium sulfate) in a hot bath! I buy 25 kilograms at the local farmers’ feed warehouse for $22 NZ. Our farmers feed it to their cattle.
Put about 1/2 kg in bath and fill with hot water. Soak yourself. The magnesium is trans-dermal (it goes through your skin) into your muscles, joints, blood….Muscles relax. Everything relaxes.
It is safe
Massage, stretching, one of those machines that zaps electricity, and ibuprofen (they did give me a prescription version). And time, warm baths with person salt then yoga when it heals more. Feel better.
Up until the early 1950s, opiates were routinely prescribed for a variety of illnesses, both physical and mental, including ubiquitous depression. Yet there seems to have been no devastating social carnage associated with that common medical practice. Demonizing opioid meds, essential for many chronic pain patients to function even semi-normally, demonstrates a lack of critical thinking. Why does contemporary society suddenly find itself unable to handle a form medicine used for centuries to treat a wide variety of ailments? THAT’S the question upon which we should be focusing.
This article could have been written after American doctors realized that their favorite cough medicine, Bayer’s Heroin (promoted as non addictive), turned out to be addicting. Whooda thunk that an opioid might be addictive? Apparently, medical schools lack a course in history.
That articles shows how factual science can be used to deceive and market something as dangerous as opiates. It is only one little piece of the picture though. It should really sparks some cognitive dissonance when they claim they “just did not know” either Physicians or patients who “Mistakenly got addicted.” The A,M.A American Medical Association counseled their member physicians physicians that it was not in their interest to take Continuing Education on either pain or addiction. The for profit medical industry discourages anything that could interfere with profitability.
The mass media failed to keep us informed, and even patient groups were subverted by Pharmaceutical Industry funding. The industries could not have patients ganging up online and exposing them, so they described the appropriate narrative. Companies like Facebook encouraged these so called communities, so they could sell their data, and generally misinform the public. The mass media sensationalized addiction related crimes, and even “Addicted Babies.” They left out facts like the number of people in the US with Chronic Pain, or the numbers of failed surgeries and misdiagnosis. Instead they targeted pain patients, blaming hem for the “Epidemic.” The Corporate profiteers behind all of this could be kept out of the narrative. It looks as if they are suing the Pharma Companies, but these lawsuits have barely scratched the surface, and the amounts are trivial compared to the profits.
That one Study was blamed, it was safer than exposing the politician who took money to subvert federal laws.
Healthcare advertising used to be illegal in this country, for good reason. Not they are using this so called epidemic as a marketing extravaganza. Fear based marketing is powerful, and nearly every quack, Pharma ad, and even the medical marijuana industry is capitalizing on that fear. Politicians who took money from the industries to look the other way are using the “opiates” in their campaign. Psychologist are cashing in too. They made a deliberate mistake in their DSMV, conflating addiction with dependence, in a careful targeting of lower income people with chronic pain. The press is still making this deliberate mistake. Sensationalism sells newspaper subscriptions, and increases advertising revenue. Cashing in is still a Bi Partisan effort!
The use of one study taken out of context has proven to be a great marketing and propaganda tool
https://www.theguardian.com/us-news/2018/may/22/rudy-giuliani-opioid-epidemic-oxycontin-purdue-pharma
https://khn.org/news/rudy-giulianis-consulting-firm-had-hand-in-halting-florida-ags-opioid-investigation/
Journalist proposed some guidlines but most ignore them, by design.
https://www.cjr.org/covering_the_health_care_fight/what-the-media-gets-wrong-about-opioids.php
Here is another misleading news article:
https://www.yahoo.com/finance/news/chart-u-s-opioid-crisis-holding-back-certain-states-183503446.html
People with chronic pain are denied pain care,
https://www.tampabay.com/opinion/columns/dont-punish-pain-sufferers/1222487
The Opiate Guidelines are being co opted by certain industries profiting from it.
https://www.cato.org/blog/new-fda-initiative-implies-cdc-opioid-guidelines-are-not-evidence-based
Another distressing but overlooked fallout from the current misguided over-reaction to the addiction crisis is that it is the poor who will suffer the most.
Recently, Medicare has essentially made prescription narcotics for the elderly unreimbursable. They will only pay for opiates needed for more than a few days in the limited case of cancer and those in hospice.
No matter how bad the pain, no matter how ineffective and dangerous aspirin and ibuprofen are, the elderly poor will have the choice of suffering or signing up for hospice–even if they are not really “terminal”–which is essentially assisted suicide, since the extraordinarily low Medicare hospice reimbursement rates preclude meaningful treatment (or even meaningful palliative care for that matter).
It looks as the link in my first post didn’t work. Here are two sites, one that summarizes the study that shows that deaths from prescription opiates have been exaggerated, and another is the study itself.
https://www.cato.org/blog/cdc-researchers-state-overdose-death-rates-prescription-opioids-are-inaccurately-high
https://ajph.aphapublications.org/doi/10.2105/AJPH.2017.304265