Yves here. This gumshoe approach to suicides is badly needed. I hope more communities take it up.
By Maureen O’Hagan. Originally published at Kaiser Health News

In 2012, Washington County, Ore., epidemiologist Kimberly Repp was asked by county officials to study suicide. She accompanied one of the county medical examiner’s death investigators on his grim rounds for more than a year. “Nothing can prepare you for what you’re going to see,” she says. (Adam Wickham for KHN)
On Kimberly Repp’s office wall is a sign in Latin: Hic locus est ubi mors gaudet succurrere vitae. This is a place where the dead delight in helping the living.
For medical examiners, it’s a mission. Their job is to investigate deaths and learn from them, for the benefit of us all. Repp, however, isn’t a medical examiner; she’s a Ph.D. microbiologist. And as the Washington County epidemiologist, she was most accustomed to studying infectious diseases like flu or norovirus outbreaks among the living.
But in 2012 she was asked by county officials to look at suicide. The request led her into the world of death investigations, and also appears to have led to something remarkable: In this suburban county of 600,000 just west of Portland, the suicide rate now is going down. It’s remarkable because national suicide rates have risen despite decades-long efforts to reverse the deadly trend.
While many factors contribute to suicide, officials here believe they’ve chipped away at this problem through Repp’s initiative to use data — very localized data that any jurisdiction could collect. Now Repp’s mission is to help others learn how to gather and use it.
New York state has just begun testing a system like hers. Humboldt County, Calif., is implementing it. She’s gotten inquiries from Utah and Kentucky. Colorado, meanwhile, is using its own brand of data collection to try to achieve the same kind of turnaround.
Following The Death Investigators
Back in 2012, when Repp looked at the available data — mostly statistics reported periodically to the federal Centers for Disease Control and Prevention — she could see that suicide was a big problem and that rates were highest among older white men. But, beyond that, the data didn’t offer a lot of guidance. Plus, it lagged two years behind.
She returned to her bosses. “I can tell you who has the highest suicide rate, but I can’t tell you what to do about it,” she recalled telling them. “It’s too broad.”
So she turned to the county medical examiner’s death investigators. They gather information at every unnatural death scene to determine the cause (say, drowning or gunshot) and manner (homicide, suicide, accident). It’s an important job, but a grim one, and it tends to attract unusual personalities.
Repp mustered the courage to introduce herself to one of the investigators, Charles Lovato. “I said, ‘Hi, my name is Kim and I was hoping to go on a death investigation with you.’ And he’s like, ‘You’re that weirdo that does outbreak investigations, aren’t you?’ And I’m like, ‘You’re the weirdo that does death investigations.’”
The gambit worked. Repp accompanied Lovato on his grim rounds for more than a year. “Nothing can prepare you for what you’re going to see,” she said. “It gave me a very healthy dose of respect for what they do.”
She studied the questions Lovato asked friends and family of the deceased. She watched how he recorded what he saw at the scene. And she saw how a lot of data that helped determine the cause and manner of death never made it into the reports that state and federal authorities use to track suicides. It was a missed opportunity.
On the wall of Washington County epidemiologist Kimberly Repp’s office is a sign in Latin: Hic locus est ubi mors gaudet succurrere vitae. This is a place where the dead delight in helping the living. (Adam Wickham for KHN)
Collecting Data On The Dead To Save Lives
Repp worked with Lovato and his colleagues to develop a new data collection tool through which investigators could easily record all those details in a checklist. It included not only age and cause of death, but also yes/no questions on things like evidence of alcohol abuse, history of interpersonal violence, health crises, job losses and so on.
In addition, the county created a procedure, called a suicide fatality review, to look more closely at these deaths. The review is modeled on child fatality reviews, a now-mandatory concept that dates to the 1970s. After getting the OK from family members, key government and community representatives meet to investigate individual suicides with an eye toward prevention. The review group might include health care organizations to look for recent visits to the doctor; veterans’ organizations to check service records; law enforcement; faith leaders; pain clinic managers; and mental health support groups.
The idea, Repp said, isn’t to point fingers. It’s to look for system-level interventions that might prevent similar deaths.
“We were able to identify touchpoints in our community that we had not seen before,” Repp said.
For example, data revealed a surprising number of suicides at hotels and motels. It also showed a number of those who killed themselves had experienced eviction or foreclosure or had a medical visit within weeks or days of their death. It revealed that people in crisis regularly turn their pets over to the animal shelter.
But what to do with that information? Experts have long believed that suicide is preventable, and there are evidence-based programs to train people how to identify and respond to folks in crisis and direct them to help. That’s where Debra Darmata, Washington County’s suicide prevention coordinator, comes in. Part of Darmata’s job involves running these training programs, which she described as like CPR but for mental health.
The training is typically offered to people like counselors, educators or pastors. But with the new data, the county realized they were missing people who may have been the last to see the decedents alive. They began offering the training to motel clerks and housekeepers, animal shelter workers, pain clinic staffers and more.
It is a relatively straightforward process: Participants are taught to recognize signs of distress. Then they learn how to ask a person if he or she is in crisis. If so, the participants’ role is not to make the person feel better or to provide counseling or anything of the sort. It is to call a crisis line, and the experts will take over from there.
Since 2014, Darmata said, more than 4,000 county residents have received training in suicide prevention.
“I’ve worked in suicide prevention for 11 years,” Darmata said, “and I’ve never seen anything like it.”
The sheriff’s office has begun sending a deputy from its mental health crisis team when doing evictions. On the eviction paperwork, they added the crisis line number and information on a county walk-in mental health clinic. Local health care organizations have new procedures to review cases involving patient suicides, too.
From 2012 to 2018, Washington County’s suicide rate decreased by 40%, preliminary data shows. To be sure, though, 68 people died by suicide here last year, so preventing even a handful of cases can lower the rate quite a bit.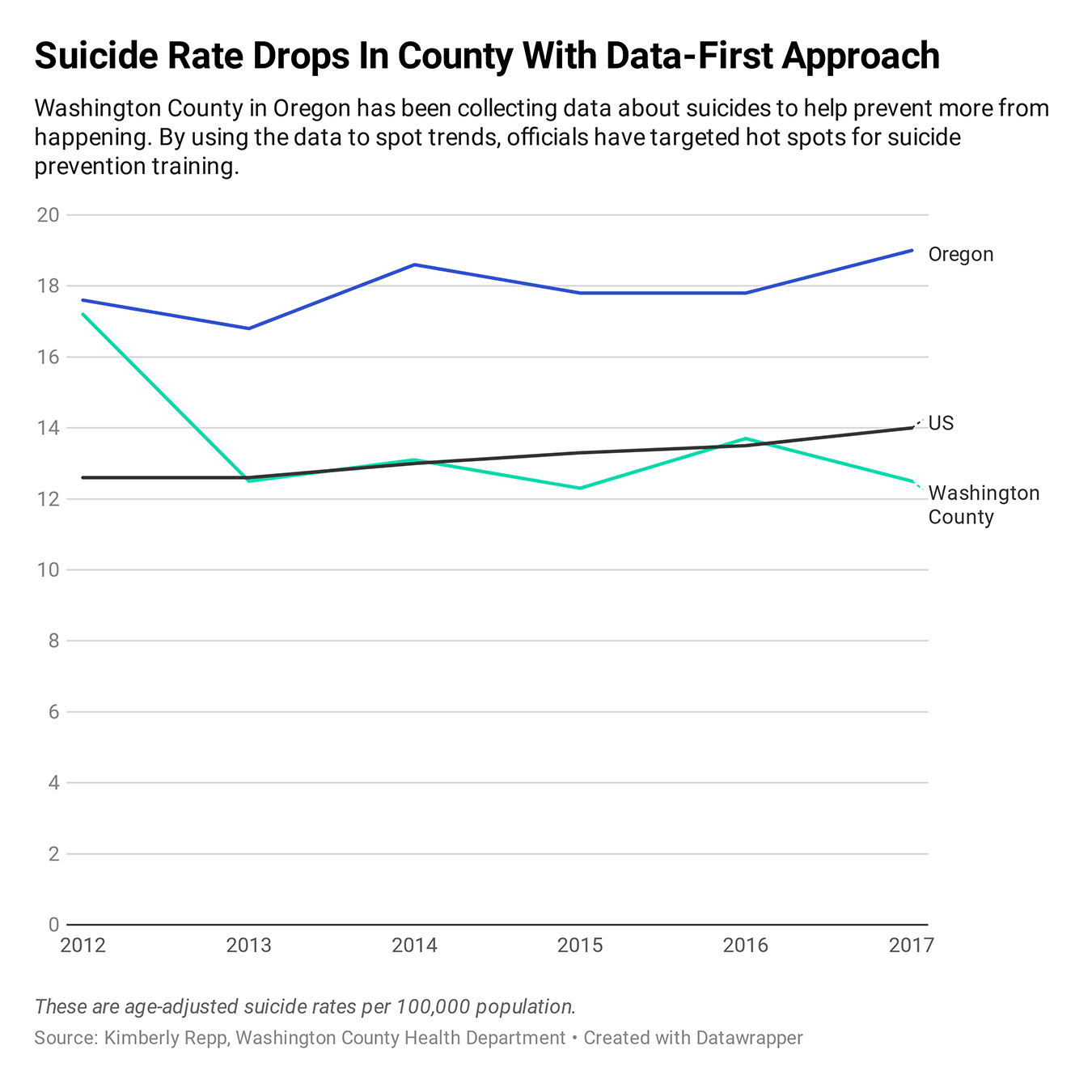
Taking The Idea Elsewhere
Repp cautions that the findings can’t be generalized. What’s true in suburban Portland may not be true in rural Nebraska or the city of San Francisco or even suburban New Jersey, for that matter. Every community needs to look at its own data.
Still, Jay Carruthers, who runs New York’s Office of Suicide Prevention, saw the potential. “To be able to close the loop and connect [the data] to prevention? That’s the beauty,” he said. This year, the state is beginning to test a similar system in several counties.
In Northern California’s Humboldt County, public health manager Dana Murguía had been frustrated for some time that local prevention plans weren’t making a dent. “I said, ‘We don’t need another plan. We need an operations manual.’ That’s what I feel Dr. Repp has given us.”
Humboldt began using a Washington County-style checklist this year, and county officials have identified several unexpected touchpoints, including public parks and motels where people have died by suicide. Now, those sad facts can become action plans.
In Colorado, a different effort to reduce suicides also began with extensive data analysis. There, they realized that while youth suicide has understandably been a focus, the biggest numbers are among older men. They’ve not only crafted materials specifically for men in crisis, but they’ve also created materials for specialized groups, such as veterans, farmers and construction workers.
“What was unexpected to me was how empowering these data would be to so many different people to make change,” Repp said — including Lovato and the other death investigators. “To know that they’re actually keeping the living alive is really powerful.”
If you or someone you know is thinking about suicide, call the National Suicide Prevention Lifeline at 1-800-273-8255, or use the online Lifeline Chat, both available 24 hours a day, seven days a week.


Tremendous level of agency here. Missing the names of the county officials who initiated and supported the work. Then implemented systemically. At evictions. At motel desks. Increasing systemic And individual agency at all levels. Think of being a desk clerk who helped prevent a suicide. Real life.
Impressive.
I wrote a book on Native suicide in Canada back in 2014 with Shaunessy McKay; we charged “murder” on the part of the Canadian government (rather than suicide on the part Native peoples) arising from Canada’s long-standing program of coerced assimilation. Mainstream psycho-social models of suicide “blame the Native victim” of Canadian policies of economic marginalization, and we noted that this line of thinking works for non-Native peoples, too. Nobody has paid any attention to our work . . . everyone is quite happy with “therapeutic interventions” based on hypothetical internal gremlins which have no basis in fact. We’ve been giving away our book at academia.edu and researchgate.net. But the relation between killing oneself and economic factors was recognized by Marx in 1845 (from translating Peuchet’s memoir’s of 20 years earlier), and these connections are manifest, not hypothetical. Maybe now that non-Indians are making our point they’ll be given some attention; who knows?
Thanks for mentioning your book, Roland. I have Lakota friends in the Pine Ridge community in South Dakota. Their addiction, murder and suicide rates are unbelievable. But, one has only to look at the cultural assimilation policies forced on the Lakotas by the government; from a tribal society, with no concept of ‘private’ property, living in closely knit communities that moved according to the seasons and food availability, they were forced to settle on widely spaced ‘homesteads.’ The sense of social isolation, as well as the dependence on vehicles (which are all old and are constantly breaking down) is slowly killing their society.
The current issue of New York Review of Books has a review of 2 books on Inuit suicide agreeing with you about forced assimilation being the cause: Too Many People: Contact, Disorder, Change in an Inuit Society, 1822–2015 by Willem Rasing, with a foreword by George Wenzel
The Return of the Sun: Suicide and Reclamation Among Inuit of Arctic Canada by Michael J. Kral
“we charged “murder” on the part of the Canadian government (rather than suicide on the part Native peoples) ”
Love this! This will help me more than you know. I am constantly looking for ways to re-frame my economic situation and suicidal thoughts and this struck me to the core. I mean, I had the thought in my head, but the thought I am being murdered…wow.
Looking for your book now…
Here’s a link to the researchgate version.
I’d avoid academia.edu – they’ll plague you for years with email enticements.
If people had meaningful work to do, as in, something that would connect them to a cause that’s larger than themselves, I think our suicide rate would go down.
This is one of the many reasons why I favor a Green New Deal.
Understandable from the point of keeping the mind occupied, but perspective is important. While some may find their job enjoying or fulfilling, part of the problem can be people over identifying all aspects of their being with work. One has to feel they are “somebody” irregardless of employment that is precarious by design in the global economy.
Keep in mind that not all depression is socio-situational. I have been suicidal doing meaningful work plenty of times. Other environmental factors will effect mood; diet, EMFs, Air Pollution, etc.
Seasonal Affected Disorder is why Oregon’s rate is so much higher than the rest of the nation. Same goes for Washington State.
Michigan’s is very high as well. We receive in lumens the least amount of light of any state.
AS, here in Boston and most of blue USA, there are plenty of opportunities to do meaningful work, like helping children or the elderly–but good luck paying rent. Decades of anti-development activism have pushed people further and further out to the periphery and hastened many evictions. We have to build urban housing and/or transportation to peripheral areas; if not, jobs (even at $15/hour! even with free healthcare!) are pointless.
Policy developers, interveners and potential suicides should consider the thoughts in the works of David Hume, Arthur Schopenauer, and even H.L. Mencken; in sizeable numbers of cases and situations, suicide is the best solution to personal misery and should be seen as a “right” regardless of society’s sense of social, economic, religious loss.
Suicide is Painless (M.A.S.H. theme song)
https://www.youtube.com/watch?v=4gO7uemm6Yo
Thanks for sharing a positive story about on a sad topic. I enjoy its narrative about, as Steve H. said, agency.
Then, and I guess this points at my general pessimism regarding the tech sector, I thought that when VCs learn about a data-driven approach to reducing suicide there will soon be apps, SAAS platforms and the rest competing to dominate rendering the data and turning it into predictions.
That Kimberly Repp is one smart person. When reading this article, I could not help but think how obvious her solutions were. But as she seemed to be the first to think of those solutions and put them into practice, that is what makes her such a smart person. It is always the obvious solutions that we do not think of.
OK so some motel clerk, housekeeper, animal shelter worker or pain clinic staff think that a person is going to commit suicide and then they call the cops. What could possibly go wrong with that situation. Cops kill more people than mass shooters in this country. Never call the cops. Period.
This is where anti-police extremism leads. The truth is that with no press attention due to victims’ privacy, the police save an uncounted number of people from suicide attempts each year. Absolutely call 911 if you know someone is about to take their own life.
And besides, who said they were calling the police? I thought they were calling a suicide prevention hotline.
Dear sweet [family blog] [family blog], this is grim: “The sheriff’s office has begun sending a deputy from its mental health crisis team when doing evictions. On the eviction paperwork, they added the crisis line number and information on a county walk-in mental health clinic.” It’s like something from the film Brazil. Department of Alienation Enforcement.
The modern, mild-mannered, rational, bureaucratic, humane equivalent of having a priest administer the last rites before they burned you at the stake.
Yves, thank you so much for posting this.
While I applaud them for their brilliant work, as you and others here know, it does nothing about the fundamental economic issues driving death by suicide.
Middle aged men have been psychologically bent to think that their power can only be expressed economically. I would rather the suicidal focus their rage collectively, and outward, and in the right direction.
“…a number of those who killed themselves had experienced eviction or foreclosure or had a medical visit within weeks or days of their death.”
Implementing interventions at hotels, motels, public parks and animal shelters is like putting salve on a suppurating wound. It might bring momentary relief, but does nothing to address the underlying infection. In these cases, the underlying wound is a predatory financial system that extracts labor, resources, hopes, dreams and finally, the very life from ordinary people.
While the idea of meaningful work has its place in suicide prevention, a more therapeutic frame involves re-imagining housing and healthcare as rights to be enjoyed by all persons in a society, regardless of income. They are not commodities, like televisions or beachside vacations. People should not be driven to the edge of a financial or emotional cliff because of impending housing losses or health crises.
The results reported in the post are impressive. That such a straightforward, eminently logical, and practical approach could prove so effective but had to wait so long for application anywhere leaves me wondering about the true motives of the many other campaigns for suicide prevention, and advertised concern for dealing with what I perceive as growing Mental Health problems. When I tried to get help for my sister when she seemed suicidal after the death of her husband, I found little behind the many suicide hotlines and the sheriff’s department said they could only help if she plainly stated she intended to kill herself or made an attempt. I finally dragged her to the only psychiatric evaluation center in the area available on a weekend — a local hospital E.R. where they helped her by wrenching her back when she resisted going in for evaluation and started loading up a fat bill for service. I wonder how much of all the concern for suicide prevention and help for mental illness is motivated by a true desire to help or more venal motives in the Medical Industrial Complex. Mental Health remains fertile area beckoning fuller exploitation of public and private funds.
There is supposed to be a high suicide rate among veterans. One way to reduce suicides is to end the wars.
Too simple. Can’t work..
So much excellent and righteously outraged commentary above, and I totally agree with the outright murder by government wording in so very many instances were now witnessing countrywide.
Would love to have been a fly on the wall of the actual conversations that transpired during Kimberly Repp’s hiring. One which may well have come up, and should have if it didn’t, is: shouldn’t we be placing abundant resources into tracking the failed suicide attempts, versus only piecing together the details after someone has died?
After all, the suicide attempts (Very tired of hearing that rural male statistic when males are far, far likelier to own guns, and guns are the most successful method) show a far, far clearer picture of the problem and the persons attempting it, since so very many suicide attempts are unsuccessful and end up with someone in an ER Unit, and then a forced Psychiatric Facility stay. At the ER unit, it seems in many cases it would be quite clear if someone was trying to lethally harm themselves via the many common methods: hanging; overdosing on meds especially those they don’t normally take; slicing themselves in certain areas; ‘trespassing’ on commuter rail tracks; surviving a fall from a bridge, or tall building. Further, those who attempted are alive to explain that: they can no longer afford to live in a non agonizing, or with physically unbearable condition without doing something criminal and would rather die.
Answering my own question as to why the exploding Suicide Attempts are not being researched –let alone made known – I’m going to say that Government VIPS are far more concerned with preventing shameful successful suicide counts amongst the ‘residents’ living under their reigns (California is quite adept at this, with their irrefutable rate of Teen suicide attempts and recorded fatalities) then they are in correcting the irrefutable social and economic conditions which have clearly been exploding quick and slow suicide attempts across the US.
When we start reading mainstream coverage of actual suicide attempts is when I’ll believe the utterly corrupted US Government-along with so many equally corrupted State, County and Local Governments – are acknowledging what a travesty (a href=https://www.nbcnews.com/health/mental-health/suicide-rates-are-rising-especially-rural-america-n1050806>From 1999 to 2016, the rate of suicide among Americans ages 25 to 64 rose by 41 percent…, I can’t even imagine what the Suicide Attempts rose by) is unraveling in the face of an increasingly rampant, predatory, deadly, corrupt, amoral technocracy and abundant wars for profit. This has created a handful of obscenely wealthy billionaires amongst an increasingly impoverished and utterly traumatized populace of millions in the US, and billions abroad.
The only reliable measure of a decrease in those who are suicidal – which should be the ultimate measure in suicide prevention – is a decrease in those who desire to kill themselves because life has become unbearable.
Corrected link referred to in the second to the last paragraph: From 1999 to 2016, the rate of suicide among Americans ages 25 to 64 rose by 41 percent… .
Too bad this conversation sunk so quickly below the horizon. There is so much, much more to be discussed about the explosion of US suicides and the much, much higher explosion of Suicide Attempts.
Further, there has been utterly no discussion, certainly not in the piece above, as to what actually happens to someone when they do seek Suicide Hotline™ help, or are referred to Mental Health Services™. That system is utterly broken, particularly when many seeking help are not mentally dysfunctional THEY JUST CAN NOT AFFORD TO LIVE, and cannot pay for the further economically crippling and job prospect destroying psychiatric lockup that may follow (or even worse, dependent on the cop[s] that arrive; yes a dwindling few are great and caring, but increasingly many are dangerous to call upon, that’s irrefutable historically, and certainly currently) if they end up on a phone line with some utterly underpaid, and unvetted responder who immediately calls 911 on them.
Even further, those who are mentally not totally functional, are treated even far more horridly, if they are not middle class (even if they used to be considered such), wealthy, or ‘prominent.’ I’ve witnessed this firsthand, over years now with some family members.
Furthermore, anyone want to lay odds on the ‘assistance’ given a homeless person when they call a Suicide Hotline™; because again, if the call person who responds refers to emergency services: that treatment (which is undoubtedly large doses of psyche meds with many times horrifying potential side effects) WILL BE BILLED TO THE PATIENT, whether they requested it, or not. I’m guessing there’s even a code for homeless callers, and they are quickly dismissed.