Yves here. In a bit of synchroniticy, at a press conference on Thursday, Trump fielded questions about the shortage of critical medical supplies, with ventilators at the top of the list. Trump blew off the notion that this was his problem. From New York Magazine:
Trump [at the Thursday press conference] argued the pandemic was a completely unforeseeable event. “No one in their wildest dreams thought we’d need tens of thousands of ventilators,” he proclaimed.
Many people thought this. Trump’s own government studied the issue and warned this past fall that it was unprepared for a pandemic. The vulnerabilities cited in the report included an acute shortage of ventilators. In recent weeks, news reports have highlighted the ventilator shortfall in increasingly urgent terms. More than three weeks ago, Health and Human Services secretary Alex Azar testified that hospitals lacked enough ventilators and other equipment to handle the coronavirus.
Hospitals and congressional Democrats have been pleading with Trump to use the Defense Production Act to commandeer industrial resources to crank out more equipment. Asked about this again, Trump shifted the responsibility onto state and local governments:
“Governors are supposed to be doing a lot of this work … the federal government is not supposed to be out there buying vast amounts of items and then shipping. We’re not a shipping clerk. As with testing — the governors are supposed to be doing it … but this is really for the local governments, governors, and people within the state, depending on the way they divided it up.
“Governors are supposed to get it. States are supposed to get it. For years, they bought ’em — and now, all of a sudden, they’re coming to the federal government.”
It is absolutely astonishing that Trump believes state and local governments should have primary responsibility for handling a national pandemic.
By Thomas Neuburger. Originally published at DownWithTyranny!
Click to enlarge (source)
There’s quite a lot to write about coronavirus, all of it of the PSA variety. There’s the coming need for hospital beds (“These Places Could Run Out of Hospital Beds as Coronavirus Spreads“), the need for parts for ventilators (“Volunteers 3D-Print Unobtainable $11,000 Valve For $1 To Keep Covid-19 Patients Alive; Original Manufacturer Threatens To Sue“), the need to understand the new working-from-home environment (“Working From Home? Zoom Tells Your Boss If You’re Not Paying Attention“), and so on.
But let’s start with ventilators.
Coronavirus-19 is a respiratory disease, “an infectious disease caused by the virus strain severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).” It is not the flu. It attacks the lungs, and those whose respiratory or immune systems are weak are particularly vulnerable to severe infections, which often result in death.
Key to keeping the death toll down for those with virulent infections is the availability of mechanical ventilators, machines that help people breathe when their lungs can’t breathe on their own. After recovery from the COVID infection, normal breathing capability is restored and the ventilator is removed. Access to ventilators is critical to saving lives in a crisis like this, more important even than hospital beds, since ventilators can be used almost anywhere — in a triage setting, for example.
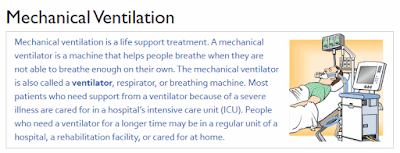
Of special importance are portable, low-cost ventilators. (Note the picture at the top, showing a ventilator in a hospital setting — not very portable, not very cheap.)
Fortunately, such a low-cost device exists, or will soon:
We need more ventilators. Here’s what it will take to get them.
As a Stanford postdoc a decade ago, Matt Callaghan created the designs for a streamlined, low-cost ventilator that hospitals could stockpile, to prepare for the possibility of a global pandemic.
But when he went to cofound a company, One Breath, he and colleagues determined the immediate need was producing cheaper ventilators for critical care in the developing world, where chronic respiratory illnesses are among the leading causes of death.
The company raised several million dollars, set up manufacturing in Southeast Asia and finally expected to begin production for its initial markets within the next 12 months.
Here’s what the new ventilator will look like; compare that to the ventilator pictured at the top.

The obstacles to retooling this device for first-world use are many, as you might imagine. “To begin manufacturing devices suited for an escalating pandemic – which entail different standards, features and batteries – Callaghan says they would need to raise additional funds, lock-in contracts and secure fast-track regulatory approvals, including from the US Food and Drug Administration” — and that just lists a few of the roadblocks.
Chief among them, of course, is money, which brings us to the “free market”:
Adding factory capacity also costs a lot of upfront money, creating real risks for these businesses, since it’s possible hospitals won’t need as many ventilators as the worst-case scenarios suggest.
“Who will pay for all the extra ventilators even if the company can ramp up?” said Kenneth Lutchen, dean of the Boston University’s College of Engineering and a professor of biomedical engineering, who is focused on developing safer mechanical ventilators, in an email. “Presumably at some point this crisis will play itself out and the hospitals will have far more ventilators than they need until the next crises.”
“There needs to be an incentivized business model to hit the go button for ramping up manufacturing and government likely needs to figure out how to successfully engage,” he added.
Who will pay indeed? “An incentivized business model” is one answer. I mean, why would hospitals pay for ventilators they need now, but won’t need later, without being incentivized? It’s only lives after all, and their investors need to eat too.
The other answer is the Sanders solution: It’s an emergency; government steps in and does the job only government can do. Government funds the ventilator company and mandates the ventilators by hospitals be purchased and made available. After all, during World War II the investment community didn’t decide how many jeeps GM would produce — GM was told what to produce and complied.
This is as true today as it was a month ago: There is no neoliberal solution to this problem. Barring a miracle cure, we’ll solve it the Sanders way or we won’t solve it at all.


Was there ever a greater opportunity than now to crush the laboring classes? Which as Groucho pointed out includes most of the ‘professional’ salaried 9% percenters.
Keep them at home with ankle bracelets on starvation stipends that can be nullified with a click of your app-based “personal account” for infractions real or imagined.
“Distributed justice” medical triage applied to the plebes at point-of-entry to hospitals; go right for treatment, go left for none. Medical advice if you think you are sick? Stay home.
UBI and JB rolled into a single hellish and never-ending debt servitude wielded by banks and their servants. Cancelled elections. Mandatory work details.
And, given the near total collapse of the democratic-electoral charade, install an Elysium-style technocratic directorate?
Hope this is a crazy conspira-theory.
They would have it said that it was not planned; they would say instead that there is no alternative; TINA
Zbigniew Brzezinski told us all about the world to come. Nothing “conspiratorial” about him.
In related news, Tony Stark wannabe continues to provide dark amusement (free registration required).
Here’s a non-paywalled version of the story:
https://finance.yahoo.com/news/spacex-tesla-working-ventilators-elon-192240652.html
As I snarked on first hearing Stark, erm I mean Musk, blathering about ventilators, “…and each ventilator will come wrapped in a brand-new Tesla Model Y! (Separate purchase required). See, that Fremont Tesla plant open really *is* an essential business – shutting it down would put thousands lives of risk!”
The Musk ventilator control software will be based on the Tesla Self Driving software. While it mostly will work well, every now and then when a Nurse passes by, it will cause the patient’s lungs to explode, by repeatedly omitting the exhale cycle of ventilation.
This Musk will explain away by stating the patent was too worked up by the Nurse’s beauty. /s
Or, to paraphrase the NTSB report about the Tesla it’s-not-really-an-Autopilot-related crash in today’s links, “the explosive chest decompression was caused by patient’s inattentiveness while breathing.”
Ventilators are not like scuba masks. They involve anesthetizing the patient and sticking tubes through the airway, often damaging the lungs (acceptable damage since you only do it if the patient will otherwise die). They’re used in ICU’s which are called that because the care in them is intensive. That is, they need a lot of trained personnel and other hospital equipment around to be useful at all. If there is a shortage of them, producing more can relieve that bottleneck (which is good), but then something else becomes the bottleneck. So yeah it’s all well and good that new economical designs are being stimulated, but it’s one component of dealing with the problem.
That said, Canada *did* stockpile 1000s of them during the 2007-8 SARS crisis and the US has a lot of them too from then. No idea why they are not yet deployed. Same thing with some millions of surgical masks.
For example, do we have enough endotracheal tubes?
The US has about 10,000 ventilators in what is called the National Stockpile. The DOD has an additional 7000. They will need a lot more than that if this thing hits at full force a la Lombardy.
A progressive TINA!
Who’d have thunk it?
I hope this crisis is not allowed to go to waste.
This crisis seems to have a left wing bias. I’m all for it. The left wing bias, that is.
Does the insistence on paying for things overrule any other consideration? Must there be a. profit for the few that the many may live? Faced with a plague which respects no boundaries, has no care for assumed status, is unaware of the size of a bank account, cares not for the place or size or magnificence of your residence, and neither knows nor cares if any individual profits, do what is needful. One purpose of government is to provide that which all need but no subset feels duty bound to provide. Since it appears that one trillion dollars can be conjured out of thin air to rescue the economy, could a few pennies not be spared to provide the means of survival.
from The Lancet, March 12, 2020: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2930566-3
In this study, a patient on a ventilator for pulmonary issues caused by cv has a 5% survival rate.
This interests me and the data science techniques they use are quite familiar to me so I looked at that article but can’t as yet find that 5% number in that context in that article. I searched for “ventil”, for “surviv” , for “rate” to find it. Can you point me to that – perhaps a quote and associated page or table that I should look in ?
I did learn about invasive and non-invasive ventilation and ventilator-associated pneumonia from the article.
from their page 5 of the article — see the two consecutive table line items for “invasive” and “non-invasive mechanical ventilation”
summing these line items — total n equals 58 in these two categories of which 3 survived
similarly, in the table, “high-flow nasal canula oxygen therapy” not great outcomes either: n=41 of which 8 survived
these are low n conclusions but it is hard to bend these numbers to get (say) 50% survival rates for these therapies
with respect
Great link, thanks.
Note that this isn’t a clean room test. A patient on an Invasive ventilator is expected to already have had or get in conjunction if they show up seriously ill all the other – antibiotics (??!!), anti-viral, etc.
Sigh. Anybody who gets to the vent stage is already dead at least in this first wave, anyway.
I have worked with Matt Callaghan in the past. He is really committed to getting the ventilator to market. His original vision was to bring it to poorer countries, but it would be nice to have now even in rich countries.