By , Head of School of Medicine, Anglia Ruskin University. Originally published at The Conversation.
Modern medicine rightly emphasises the importance of science. The focus, however, too often displaces our attention from the real point of healthcare – to care. This is nicely captured by William Osler’s (1849-1919) admonition to attend to the patient rather than their disease – a sentiment treated as a quaint bromide by the unwary practitioner. I rediscovered the truth of his advice when two particular patients taught me about COVID-19 infection and challenged what expertise I thought I had in managing pneumonia.
The first patient with COVID-19 that presented to my hospital was probably typical of initial patients in many other hospitals at the time. He was an elderly man with pneumonia, as yet untested for the new coronavirus but presumed to have it. An expert team carefully assessed him, prescribed high-flow oxygen and monitored him on a respiratory ward. He died unexpectedly that night.
The second patient was a middle-aged woman referred to the intensive care unit for mechanical ventilation. The recent death had made me nervous, so I went to assess her. On my way to the ward, I imagined the picture that awaited me – a patient gasping for air, barely able to speak, chest heaving with the effort of trying to drive oxygen into her blood.
When I arrived decked out in full PPE and ready to sedate her for immediate ventilation, I thought I had arrived at the wrong bed. She sat comfortably on her chair, speaking on her mobile phone to her daughter, bemused by my appearance. Overcautious colleagues, I thought, but measured her blood oxygen saturation just in case, more from instinct than concern. From her appearance I expected it to be close to normal (100%). It was 75% – a level barely compatible with being conscious.
Silent Lung Damage
I quickly learned that many patients with advanced COVID-19 disease bore none of the hallmarks of severe respiratory illness until they suddenly collapsed and died. The science behind this early lesson is now emerging, with a study from Wuhan, China, describing pathological lung changes on CT scans of completely asymptomatic patients. Asymptomatic carriage is not uncommon in other virulent infections, such as MRSA and C diff, but what is striking with SARS-CoV-2 (the virus that causes COVID-19) is that it may be accompanied by underlying organ damage.
The researchers found lesions consistent with inflammation of the underlying lung tissue (ground-glass opacities and consolidation, to use the medical jargon), which are not specific to SARS-CoV-2 infection and may be seen in many other forms of lung disease. What remains a mystery is why, despite these changes, patients do not display typical symptoms of pneumonia, such as severe shortness of breath.
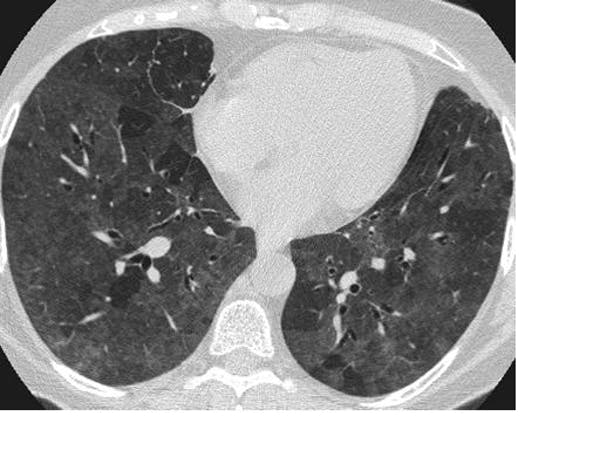
CT scan showing ground-glass opacity. Mluisamtz11/Wikimedia Commons, CC BY-SA
About a quarter of the patients in the study developed a fever, cough and shortness of breath – but many did not. The idiosyncratic response to infection is one of several conundrums of COVID-19, such as why it targets certain groups and not others – two people with exactly the same demography and health may express the disease at opposite ends of the spectrum. The study reinforces that absence of symptoms does not imply the absence of harm.
The Risks
Lack of symptoms in the face of active pathology carries a risk both to infected individuals and to the public. Current advice encourages patients to stay at home if they are asymptomatic, making late presentation to hospital and sudden death a distinct risk.
And then there is the public health nightmare. As many as 40-45% of people infected with SARS-CoV-2 remain asymptomatic, with a viral load as high as those who are actively ill. Add to that the significant false-negative rate of up to 20% for screening tests – where people are wrongly told they don’t have the infection – and the scale of the problem is magnified. These are the covert transmitters who continue to shed the virus for up to 14 days and it raises clear questions about the effectiveness of the testing strategy or the use of screening measures such as temperature checking.
William Osler, one of the founders of Johns Hopkins Hospital. Gilbert and Bacon/Wikimedia Commons
Fragments of evidence are slowly being pieced together, mainly from many small, disparate studies. The full picture will coalesce as the quality and quantity of evidence expand and refines our understanding of SARS-CoV-2. However, science still falls short of informing doctors about how to best manage the patient before them.
Lesions on a CT scan cannot determine what treatment is needed. It still requires a personalised decision based on clinical judgement. So even as scientific understanding grows, I will apply Osler’s advice with renewed conviction: attend to your patient with all five senses at full alert. They will teach you what you need to know.


I’ve read enough, especially here and at links from her, to have seen many things suggested or claimed as symptoms of COVID-19. Now, after reading this commentary in particular, I feel a growing urgency to ask . . . what does “asymptomatic” really mean? What are considered the “official” symptoms? If we have a financialwindfall, should we be donating pulse oximeters for our local hospitals and clinics, plus one for at
“. . . links from HERE, . . .”
And yes, “financial windfall” IS two words.
(Sorry about the typos — preschooler woke me up an hour and a bit ago.)
Maybe I should have waited for this morning’s Links . . . where Jerri-Lynn has kindly put in this article:
https://www.statnews.com/2020/06/26/from-nose-to-toe-covid19-virus-attacks-like-no-other-respiratory-infection/
It even links to a CDC “Symptoms” page! Thank you, Jerri-Lynn!
Glad you found the link useful.
Asymptomatic when compared to the symptoms of a typical respiratory illness. But one hypothesis is that covid-19 is more of a blood disease than a respiratory illness. This may explain symptoms such as a dry cough and loss of smell without an increase in phlegm or nasal congestion. Not to mention organ, tissue, nerve and brain damage.
When asymptomatic patients on the Diamond Princess were given a ct scan 54% were found to have lung damage. It would be interesting to test asymptomatic patients for signs of heart, kidney and reproductive organ damage as well as brain damage.
Dr. Richard Levitan who is one of the gurus of Emergency Medicine, especially in the area of ventillatory support, has recommended that patients with mild to moderate symptoms and no comorbid risk factors be sent home with a pulseox to self quarantine and monitor, returning for a saturation less than 90%. (see here: https://www.nytimes.com/2020/04/20/opinion/sunday/coronavirus-testing-pneumonia.html for a non-technical review)
Be aware that this was at the height of the New York Pandemic, where being in a hospital was dangerous by itself.
My institution has a number of portable pulse oximeters, and a plan to give them to patients should we need to slow the rate of admissions. I would advise you to contact your local hospital, and ask if you can speak with an Emergency Physician (or the director of the department) to see if they would be well received.
Silent lung damage, silent pneumonia, silent transmission reports today El Pais (Spanish), saying that the Spanish HC authorities estimate that only 1/3 of contagions surface in statistics and countries that have devoted resources to detect as much as they can, like SK, see that the disease still spreads under the radar highlighting that surveillance is needed but cannot avoid such silent spread. I think that Chinese data are simply unbelievable and under the radar spread sometimes surfacing might not be sufficiently reported in this country in which the leadership is engaged in their PR that a strong leadership is able to control the disease. Cases that cannot be linked by disease tracing methods with other previous cases abound.
Of course, if one is asymptomatic (until it’s too late), why would you get tested? That’s a real problem. And then, as noted in the article, about 20% of the tests (I’ve heard even more) aren’t accurate.
It would also be interesting to see if that kind of lung damage statistically shows up in young people if they are asymptomatic, or if this tends to be a problem still largely facing those who are 65 years old and older.
Well you might think you had been exposed and want to self quarantine before you infected others. That logic would get me tested.
Sounds to me like the really big question here is ‘can this happen to the lungs of even pre-middle age asymptomatic youngsters who think they are invulnerable’ (and can attend Trump rallies and party without consequences?
Trump rallies cause the virus but rioting, looting and protests don’t?
They give out free shots in Chicago every weekend.
This isn’t about causes. It’s about what happens to you after you have been infected if you are asymptomatic. I’d throw in people who seemingly only have mild symptoms. But since you ask, I’m guessing it is easier to social distance when you are rioting, looting or protesting than it is when you attend a Trump rally.
There has been no spike in COVID cases in Seattle after the protests because most of the people protesting were wearing masks, and were outdoors. Contrast to Trump rallies which are indoors and no one wearing masks.
The smaller spikes in NYC, Seattle, Detroit and Bay Area could easily be higher seroprevalence & FAR lower active infection rate (especially, among “essential workers,” tantamount to a racist epithet, now?) A friend texted graduation pix of happy Yemeni immigrant kids in Lansing, which was just as scary as anything we’d seen in the UWS, in March. No masks, totally ignoring their very vulnerable loved ones. All screaming into phones, planning meet-ups. We’d only achieved 23% recuperating populace (largely “minority” gig/ 1099 workers who’d managed the 24K death rate, under reported, well into April). So, we see kids here, maskless in denial that we’ve attained little, if any, immunity or antibodies. Mid America is simply naive, so to speak? But, the Market’s up!
Interesting information if true, but it seems that with such a proliferation of rushed studies there’s one to support every position. The article refers to a single study. If I’m reading the linked summary correctly, the study group was small (58 subjects) and consisted of patients who were hospitalized with COVID pneumonia, which may not be a representative sample of asympotomatic infected persons as suggested by the headline.
Similarly confused. And not enough of a science background to fully grok pre symptomatic vs. asymptomatic.
In my ignorance, I’m still staying home, washing my hands, keeping the house clean, and wearing a dang mask when out. Baffled by the number of 4th of July celebration invites coming my way.
I also have a hard time swallowing this. If significant damage to your lungs is occurring, they are saying you might not experience anything different? I mean it’s possible I guess, but I think I’ll remain agnostic for now. There are so many different things being said, and with so many agendas attached to the information I really can’t tell what is real right now. It’s like this huge smoke screen around the whole topic. Clear, concise and factual information is what I’ve been craving for…. months now.
When you say: “Clear, concise and factual information is what I’ve been craving for”,
you clearly mean: “Written words that say what I want to hear”.
There aren’t that many different things being said, and given that we’re still learning how the disease and the virus itself work, there’s bound to be some fogginess and things that come up later on. Such is the nature of research: you know nothing, then you know a bit, then know a bit more, etc. There’s no “I didn’t know anything yesterday, today I know everything there’s to know”. Knowledge is learnt progressively, the more complex the subject, the slower you learn, and biomedicine is an extremely complex topic.
That said, organ damage in asymptomatic people is well documented in a variety of studies from different sources. We might not be sure about it’s prevalence just yet, or specifics about its demography, but I think it’s safe to say that it does indeed happen.
This may be rare, but it’s far from being the only disease that causes damage without symptoms. Sometimes long-lasting damage that leads to severe problems later in life (think HPV & cervix and throat cancer).
Weird that this article referred only to Wuhan. On the Diamond Princess, over 50% of the asymptomatic cases studied showed lung abnormalities.
https://www.healthimaging.com/topics/diagnostic-imaging/ct-covid-19-lung-diamond-princess-cruise-ship
The study:
https://pubs.rsna.org/doi/10.1148/ryct.2020200110
So this is not an isolated finding.
Also note that if you read the scientific study linked, almost all of the lesions improved/disappeared during the course of the illness except in the case of a small, significantly more elderly group of patients. The headline of the original story leads one to believe that there is a very real danger, and in fact a likelihood, of anyone and everyone having lung damage whether you ever even know if you get COVID-19 or not. That implication is simply not born out in the science presented.
You are misrepresenting the study. Lesions were present in only 20% of the asymptomatic cases. Their main subclinical abnormality was consolidation, not lesions, so focusing on that is a misrepresentation. More seriously, I see nothing that says that lesions got better either. The paper does mention that perhaps the asymptomatic cases had been symptomatic and they caught them in healing phase, but they then undercut that by saying what they see in the asymptomatic CTs isn’t characteristic of what they know about Covid-19 recovery. I searched on “lesion” and there is nothing consistent with your assertion, and the tables do not show changes over time.
“attend to your patient with all five senses at full alert”
Why, as an old school primary care doc, I think telemedicine is a harmful fantasy perpetrated by the MBA’s and techbrodudes.
I don’t think telemedicine is a cure-all. If I’m seriously concerned about my health I want to be face to face with the Doc. However, an appointment with my PrimCare physician can be two weeks out. The current use of telemedicine is just a palliative for the current demand on healthcare facilities. (And the shortage of PrimCare docs.)
Using the limited video and microphone capability of my laptop to communicate is not ideal. I’m sure there is value in getting a health professional to see and talk to me online quickly, but it is not an application of the five senses. So, if health symptoms of concern present themselves I go to Urgent Care and wait (longer than I would like).
PS. Urgent Care seems to be viable profit/care centers. My local hospital is opening TEN of them.
Amen, Parker. And a huge thank you to Jeri-Lynn for this.
I think Science is broken. I have trouble believing the Corona test is well-designed. It’s ease of application, the speed of obtaining results, cost, and accuracy all leave something to be desired. Is this really the best that Science can come up with? And while billions of dollars chase after a silver bullet vaccine, how much effort has gone into learning how Corona spreads from person-to-person and learning details of how it enters, first infects, and spreads through the body. Several months into Corona and thousands of deaths and only now are we discovering that this ‘respiratory’ flu affects other organs throughout the body? How much does the guidance from our CDC and from the WHO reflect Science or even clear thinking? How much does it reflect the ‘right’ answers to please Government?
+1. There seems to be a serious problem with the way “the market” spreads incentives around in modern capitalism. I am glad to see a report on damage to asymptomatic patients, but why is there so little of it? It’s as if the press gods think certain wealthy patrons would be better off if nobody pays attention to the largest amount of damage being done. “It’s no worse than the flu.”
Apparently, in the UK, they are training dogs to smell for the virus. Seems dogs have unique abilities in this area. If my CV19 test showed negative, but the doggy wagged it’s tail, I’d take the doggy any day.
Jawb one is don’t get it.
There is no jawb two if jawb one isn’t done first.
Still flying + still partying + still mass gatherings . . . = Total Fail.
I wish some reporter would have asked Pence how he spells ‘freedumb’.
Almost six months into this thing and very few answers to an ever expanding volume of bad news. It was not treated seriously enough when it started and now is being wished away by Trump. Trump adds to the disaster by shunning masks and encouraging his followers to do likewise. It is over the top.
This virus gives new meaning to the phrase “bad breath”. Jawb one is don’t get it.
The majority of people “getting it” are “essential” workers. Many live relatively crowded home lives and have little savings. Staying home is not an option. (The bar hoppers are ‘nother story… total Fail!)
That’s just the thing. My partner and myself were obviously infected around Mar 10th in the UWS. Both, wearing proper PPE and avoiding MTA after mid February. We had no fever but few symptoms (she had a cough, I had anosmia, we both had odd, pro-inflammatory cytokine symptoms, but passed day 10, knowing this wasnt influenza (our vaccination was (typically) pretty useless, but we’d apparently had this year’s strain, previously? We’re in our late 60s). Just about the time, we’d figured it was time to start logging temperature, to verify we were safe to venture out, we each started getting scary, but very sporadic shortness of breath, burning sensations in trachea, heart lungs, joints and gut. We’d been taking several phyto-polyphenol iso-flavonoids (eg: Quercetin, Resveratrol) and cut back on Sambuchus nigra, D3, zinc) but, the Drs said no work-up or imaging & told us to delay ELISA IgG, since these were undependable, at that time. Now, our Abbott immunosurvey has us both as negative, so… it’s no major problem to avoid loud, drunked-up churls. But, it’s VERY spooky to live through a particularly stereotypical Irwin Allen version of Naomi Klein’s “Shock Doctrine,” where specious obliviousness, obdurate denial and sneering projection are the real deadliest pandemic.
I forget where I read/saw this, probably at MedCram ( a really useful youtube site, the Dr there is an excellent teacher/explainer), but the reason that CV patients can be “happy hypoxic” is that the body uses CO2 levels, not O2 levels, to determine respiration capacity.
For whatever weird reason (and he does explain it), the lung damage doesn’t inhibit removal of CO2, but it does inhibit O2 transport. Hence, “happy hypoxic”.
Buy a pulse oxymiter, they arent’ expensive. Test your self regularly. Even if it isn’t terribly accurate it should be repeatable enough to detect a trend. If you get below around 92% or so on repeated readings, it would be good to talk to a Dr, no matter if you have a cough or not.
92% is not an absolute. 92% can be on the low end of normal for someone with COPD.
And having a drink can temporarily depress your O2 levels.
But I agree 100% with getting a blood oximeter and checking daily.
On the subject of blood/O2 levels, NO or nitric oxide, is produced in the nasal passages and then down into the lungs, where it has a dilatory effect on the blood vessels in the lungs. Just by humming and nasal breathing one can maintain 99/100%, humming increases the amount of NO produced.
In the West, molecular data collection for covid is a sad joke (I’ll spare you the mini-lecture), even though such capacities do exist. The clinical observations and publications have been more useful, but without adult-level rigor at the molecular end, clinicians are still on the phenomenological back foot.
But please note–Modern medicine emphasises the importance of profit, not science. To suggest otherwise draws attention from the real point of the thing we euphemistically call US healthcare – social control. Analogous to Pollan’s “food-like substances”, we suffer through actuarialized “care-like processes” even when we are allowed “access”, the outcomes of which are fairly well characterized.
This continuing national disgrace and the current enduring display of total institutional incompetence is only obscure to a population rendered wholly unable to interact meaningfully with political, let alone biological, realities.
The prediction now is for continuing programs of propaganda and sales plans.
“The researchers found lesions consistent with inflammation of the underlying lung tissue (ground-glass opacities and consolidation, to use the medical jargon), which are not specific to SARS-CoV-2 infection and may be seen in many other forms of lung disease.”
The author just debunked themselves with the above. If these lesions are common in many other illnesses, then it cant be certain that the lesions are necessarily due to covid asymptomatic infection.
There is nothing scientific about this article. Its comparable to something one would find on ZH. And using as primary sources anything from Wuhan is just comical.
Sorry, you are wrong re Wuhan. China’s version of the CDC published a study with extensive analysis of their at the time >150,000 confirmed cases. That IIRC was back in March. It was comprehensive detail on everything they had at the time. Has the US or any country done anything even remotely approaching that?
Ground glass opacity in a suspected covid case is enough for a presumptive diagnosis, in the middle of an outbreak. Various countries restated their case figures to include clinically diagnosed as well as nucleic-acid tested, given testing issues. Its another example of treat the patient (the clinical picture) not the disease.
The Wuhan clinical papers look sound to me. They foretold of the disaster coming and are the reason my household went into lockdown in early Feb. Aerosol transmission, gi symptoms, lack of fever, anosmia, coagulopathy, kidney failure, asymptomatic spread – these are all in the early papers.
Thanks. This article got me to dig out a pulse oximeter from China that was forgotten in my quarantined goods. 98%. What a relief. Insomnia, anxiety, allergies and old age are a bad mixture. When I woke up on a ventilator at the VA, an experience I want to avoid again, I noted how treatment was by the cookbook. I am not sure they knew why they did things that they did. I was kicked out onto the street ASAP. And, this wasn’t a for-profit hospital. All the newly hospitalized in hot-spots are sure to be receiving horrendous medical bills for what ever the government doesn’t pay for. I have no idea what is and isn’t covered now. If you get out of the VA alive, at least it is free.
Coronavirus response has been politicized. Science dumped. Messaging jumbled. Both parties are focused on re-election, keeping the money coming in; not defeating the epidemic, not caring for the sick.
I am sure the vulnerable are lowering their risks as much as possible. The increased infection rate but apparent lower mortality is likely age related. The media is hyping the deaths for the ratings but not giving out information that saves lives. If there was a coordinated response, the possibility of adverse consequences for asymptomatic coronavirus infected individuals would have been determined by now. But since there is no money in it, science is on a backburner.
On the subject of blood/O2 levels, NO or nitric oxide, is produced in the nasal passages and then down into the lungs, where it has a dilatory effect on the blood vessels in the lungs. Just by humming and nasal breathing one can maintain 99/100%, humming increases the amount of NO produced.