By Lambert Strether of Corrente
This post will be a little disjointed. First, you might grab a cup of coffee and listen to this panel (“Medical Grand Round”) put together by Robert Wachter, chair of the Department of Medicine at the University of California, San Francisco. Wachter runs an excellent Twitter account, focused on #COVID19. The panel and topics:
- Aerosol vs. Droplets: Don Milton, Professor, Environmental & Occupational Health, University of Maryland School of Public Health
- Masks: Monica Gandhi, UCSF Professor of Medicine; Associate Chief of Division of HIV, Infectious Diseases, and Global Medicine at ZSFG; Director of the UCSF Center for AIDS Research; and Medical Director of the HIV Clinic, Ward 86, ZSFG
- Face Shields: Michael Edmond, Chief Quality Officer and Associate Chief Medical Officer, University of Iowa Health Care; Professor of Medicine, Division of Infectious Diseases, University of Iowa Carver College of Medicine
There is a detailed table of contents with Time Codes at the videos’s page; the video lasts a little under an hour-and-a-half. Here it is:
I like this video so much for a few reasons: The focus on masks, shields, and aerosols helps me decide what I can do to be and feel safe, in my personal practice; moreover, I stan aerosols (and not fomites). Further, all the presenters give me the feeling that they are medical scholars, and not academic entrepreneurs, dying to get into the business school, or make money ramping some stock. To me, as a child of scholars, that’s very reassuring, and it gives me hope for the world (if not necessarily hope for the United States). And all the presentations are impressive. There is even a masked cat from the 1918 Pandemic!
So if you have by now engaged in a process of caffeination and pressed the Play button, now let me pivot to the second aspect of this post, which you can possibly even multitask and read while listening. I had noted this slide by Professor Ghandi at 43:05:
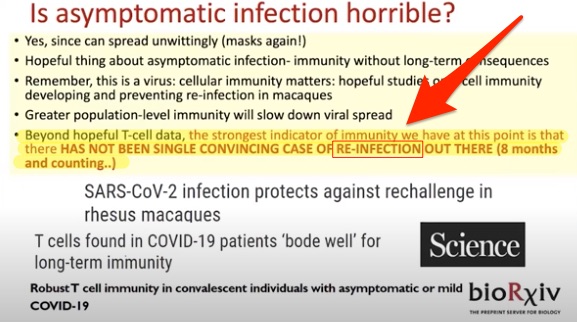
Considering the slide, I realized that there are probably some readers who would disagree on reinfection; and I realized further that I didn’t know what I would say to them. So I thought I would aggregate what I could find on reinfection and try to make sense of it.
First, there doesn’t seem to be a lot of published work on reinfection as such, if one rejects reinfection-adjacent topics like immunity. This search on “covid reinfection” at medRxiv, the preprint server, yielded exactly one hit with “reinfection” in the title; the National Institutes of Health did better, with three hits on the same search. One of them is from the Director’s Blog, so let’s start there. From Dr. Francis Collins, “Study in Primates Finds Acquired Immunity Prevents COVID-19 Reinfections“:
There have been rare reports of people recovering from infection with SARS-CoV-2, the novel coronavirus that causes COVID-19, only to test positive a second time. Such results might be explained by reports that the virus can linger in our systems. Yet some important questions remain: Is it possible that people could beat this virus only to get reinfected a short time later? How long does immunity last after infection? And what can we expect about the duration of protection from a vaccine?
A recent study of rhesus macaques, which are among our close primate relatives, offers relevant insights into the first question. In a paper published in the journal Science [here], researchers found that after macaques recover from mild SARS-CoV-2 infection, they are protected from reinfection—at least for a while.
Since the second viral challenge took place just 28 days after the first infection, this study provides a rather limited window into broad landscape of SARS-CoV-2 infection and recovery. Consequently, it will be important to determine to what extent a first infection might afford protection over the course of months and even years. Also, because the macaques in this study developed only mild-to-moderate COVID-19, more research is needed to investigate what happens after recovery from more severe COVID-19.
Of course, macaques are not humans. Nevertheless, the findings lend hope that COVID-19 patients who develop acquired immunity may be at low risk for reinfection, at least in the short term. Additional studies are underway to track people who came down with COVID-19 in New York during March and April to see if any experience reinfection. By the end of this year, we should have better answers.
(This is the macaque study to which Ghandi referred.) Collins is moderately re-assuring, but I also picked up a saying in my travels on animal studies: “Mice lie, and monkeys exagerrate.” Needless to say, if all the study proves is that reinfection is avoided only for 28 days, and that’s an exagerration, it’s hardly encouraging.
As for the other articles, the medRxiv hit is a mathematical model, as is the first NIH article. The second NIH article is a letter to the editor. The third is a restatement of the macaques study. So, with the scanty literature out of the way, let us turn first to anecdotes, and then to commentary. (As with so much #COVID19 literature, we know so much and so little at the same time.) Ordering them by time of publication:
Anecdote #1: “Questions raised over COVID-19 reinfection after Japanese woman develops illness again” Japan Times (2020-02-28):
The Osaka Prefectural Government said Wednesday that a woman in her 40s from Osaka tested positive for COVID-19 after what appeared to be a recovery earlier in February.
According to the prefecture, the woman first tested positive on Jan. 29 after joining a tour in which visitors from the Chinese city of Wuhan — where the virus is thought to have originated — also took part. She was discharged from the hospital on Feb. 1 after her condition improved. The woman tested negative during a monitoring period a few days after her release, but she was still symptomatic. She tested positive again on Wednesday after multiple visits to the hospital.
Anecdote #2: DOUBLE BLOW Diamond Princess coronavirus cruise victim ‘tests positive for a SECOND time two weeks after all-clear The Sun (2020-03-16):
A Japanese man who appeared to have recovered from coronavirus tested positive again less than three weeks after he left a medical facility where he was being treated.
The Japanese man who is in his seventies first tested positive February 14 while aboard the Diamond Princess cruise ship during its quarantine.
He was then disembarked and put in further quarantine at the medical facility in Tokyo, getting the all-clear on March 2, according to Japanese news agency NHK.
He returned home to the Mie Prefecture, within the Kansai region, via public transport, but he began showing symptoms of the virus again and developed a fever of 39C on Thursday, March 12.
He went to a hospital for a re-test and was confirmed positive on Saturday, March 14.
* Anecdote #3: Israeli woman possibly reinfected with coronavirus post-recovery Jerusalem Post (2020-05-06):
A woman who had recovered from the coronavirus was re-hospitalized a month later after testing positive again. Last week, the 45-year-old woman from Jisr e-Zarka was re-admitted to Hadera’s Hillel Yaffe Medical Center, where she was initially hospitalized with fever and chest pains. This comes a month after she was discharged from the medical center having recovered from the virus and testing negative twice.
* Anecdote #4: Recurrence of COVID-19 after recovery: a case report from Italy Infection (2020-05-16). Of all the anecdotes, I think this is the most “convincing,” because of the (seemingly) thorough-going testing:
Here, we describe a case of reactivation of COVID-19 registered in Italy at the beginning of May 2020…. After 14 days the patients became afebrile and his respiratory symptoms disappeared. The chest X-ray showed only blurred areas of parenchymal thickening. Our hospital required two consecutive negative SARS-CoV-2 molecular tests, plus normal body temperature, resolution of respiratory symptoms, with the improvement of lung imaging. The two nasopharyngeal swabs collected on March 30 and 31 were both negative for SARS-CoV-2 infection. The patient was therefore discharged and encouraged to maintain home quarantine for at least 14 days…. The molecular test was also negative at his follow-up visit on April 15, suggesting that the patient was cured from COVID-19. In addition, two serological assays (VivaDiag™, VivaChek Laboratories, INC, USA and Anti SARS-CoV-2 ELISA IgG Test, Euroimmun, Lubeck, Germany) revealed the presence of IgM and IgG anti-SARS-CoV-2.
However, on April 30, he developed new symptoms, i.e., dyspnea and chest pain. The molecular test was also negative at his follow-up visit on April 15, suggesting that the patient was cured from COVID-19. In addition, two serological assays (VivaDiag™, VivaChek Laboratories, INC, USA and Anti SARS-CoV-2 ELISA IgG Test, Euroimmun, Lubeck, Germany) revealed the presence of IgM and IgG anti-SARS-CoV-2. However, on April 30, he developed new symptoms, i.e., dyspnea and chest pain. … To the best of our knowledge, this is the first published report describing a reactivation of COVID-19 in an apparently cured patient in Italy.
Anecdote #5: As coronavirus cases soar, doctors and patients wonder: Is it possible to get reinfected? NBC (2020-07-14):
Sherry Wellman, 56, of Youngstown, Ohio, and her doctors had assumed it would last longer than two months.
After an initial positive test for the virus in March, two additional COVID-19 tests in April were negative. It was welcome news to Wellman, whose job as a nurse required her to have two negative tests before returning to work.
But a month later, she had to go to the hospital for chest pains, and was tested again.
The physicians “ended up testing me for COVID just for the heck of it,” Wellman said. “Sure enough, it came back positive. They were stunned.”
“The nightmare of this is based on how much we don’t know,” Saag said. “COVID is brand new. We’re discovering as we go.” A growing pool of data, he said, suggests COVID-19 antibodies wane about 60 to 90 days after infection….
“That’s certainly consistent with other coronaviruses,” Derek Cummings, an infectious disease epidemiologist at the University of Florida, said. Other coronaviruses include the viruses that cause SARS and MERS, as well as several that cause common colds.
But because coronavirus infections can often occur without symptoms, “it really takes careful follow-up of individuals to detect that second infection,” Cummings said.
There are three possible explanations for Wellman’s second round of positive COVID-19 results. Either her negative tests were faulty; the virus remained hidden in her system undetectable by tests before flaring up again; or she really was infected a second time.
Anecdote #6: “Coronavirus patient tests positive for a second time but that doesn’t mean she was reinfected, expert cautions” CNN (2020-07-17):
Shelby Hedgecock [a wellness coach in Los Angeles] thought a negative Covid-19 test meant she had recovered from her initial infection. But three months and another positive test later, she told CNN she is still feeling unwell. Hedgecock first tested positive for coronavirus on April 20. On May 9, she tested negative, she said.
Nearly two weeks later, she took an oral and nasal swab test. The oral test came back negative, but the nasal came back positive.
A week later, another test was negative, she said.
And still she feels symptoms, she said. Any exertion can put her in bed for days, and she is now on medication for daily headaches, she said.
It’s not clear that the second positive test means Hedgecock was infected again. It’s possible she initially received false negative test result or that the positive was misleading, CNN’s chief medical correspondent Sanjay Gupta said.
“We are not getting documented cases of reinfections yet … That’s not to say they won’t come,” Gupta said. “If people were losing their immunity I think now, six months into this, we would be seeing significant amounts of reinfection.”
Some types of coronavirus tests have a 15 to 20% false negative rate, he told Cuomo Wednesday.
“If that’s the case, then people have been walking around with a false sense of security for a long time,” Hedgecock said. “And that’s a problem.”
Testing positive after an infection could come from the test looking for genetic material of the virus, Gupta said. The genetic material identified could be a sign that the virus is present, or it could be debris the virus left behind, he said.
Anecdote #7: Israeli doctor reinfected with coronavirus 3 months after recovering Jerusalem Post (2020-07-19):
A doctor at Sheba Medical Center in Tel Hashomer tested positive again for the novel coronavirus three months after initially recovering from the disease.
The doctor “tested positive again because she has remnants of her first virus still floating around in her body,” a hospital spokesperson told The Jerusalem Post on Sunday.
The doctor suffered from fever, cough and muscle pain when she tested positive for the virus in April, but she recovered and tested negative in May and June.
Earlier this month, she came in contact with a confirmed patient and subsequently tested positive for the virus.
(There are also aggregated cased of reinfection in South Korea, but those may also be due to false positives. The same is true for China.)
There may be more cases out there[1], but those are the ones I can find with online search, such as it is. It’s impossible to know whether my search was exhaustive, or representative. (Would re-infecttion in the immigrant population of Chelsea, MA be deemed worthy of coverage?) That said, all the cases but two (asterisked) share a common characteristic: The initial infection took place in a bat cave or petri dish: A tour to Wuhan (#1), the Diamond Princess (#2), a hospital workplace (#5), a gym (#6), and a second hospital workplace (#7). Speculating freely: If we believe dose-response affects the initial infection, as Dr. Ghandi urges, it might also lead to vulnerability for a second. That would imply that the danger of re-infection is less for the general population. Seven cases, after all, is not very many — especially since the “curves” do not seem to have been affected — at least so far! (It would be really unfortunate if such immune protection as there may be wore off in time for, say, school to start.)
I’ll close on an optimistic note with the following from Popular Science, “Why no one knows if you can catch COVID-19 twice” (2020-07-16):
However, the fact that the world has seen more than 13 million known cases of COVID-19 since late 2019 and there aren’t yet any confirmed, clearly documented cases of reinfection in peer-reviewed medical journals may be telling, [Luis Ostrosky, a professor of infectious diseases at McGovern Medical School at the University of Texas Health Science Center at Houston] says. “This would lead us to the conclusion that this would be a rare event if it happens at all.”
And:
Generally speaking, it’s unusual for a virus to infect people again after a brief period of time, both Ostrosky and the La Jolla Institute researchers agree.
A number of viral diseases—including measles, mumps, and chickenpox—typically lead to lifelong immunity. But in other cases, the immune response our bodies mount to a virus isn’t strong enough to ward against reinfection; respiratory syncytial virus is one such pathogen.
Some viruses, like the ones that cause the seasonal flu, also mutate so quickly that you might recover from one strain only to encounter another that is different enough that your body’s immune system doesn’t recognize it. So far, the coronavirus that causes COVID-19 doesn’t appear to be mutating especially rapidly or in ways that would hinder vaccine development.
Finally, don’t let down your guard:
For now, though, there are two things we can do to deal with all the uncertainty.
“One is to follow the ‘Hitchhiker’s Guide to the Galaxy’ mantra, which is don’t panic,” Ostrosky says. “We need to get more information to see whether this really happens or not and if it’s a common or rare event.” Further, researchers still need to better understand whether an individual who has some immunity can still spread it to others. So if you have recovered from COVID-19, you should still be social distancing and wearing a face mask when you plan to come into contact with other people.
And even if it is an aerosol, keep washing your hands! And I hope you enjoyed the video.
NOTES
[1] Missed this one — again, there’s been no aggregation! — but the patient’s occupation is not given in any case.


Thanks for this post, Lambert!
A little cheering, that Popular Science article.
+1. The video is great. Gandhi gives good reasons to think that mortality will be much lower in the second wave in the US and the % of symptomless or nearly symptomless may be much higher. One of the reasons is the use of masks that reduces virus shedding and virus uptake –> lower viral loads, lower severity. There are other factors in play (healthier mucosae in summer, more vitamin D…) so do not expect those mortality rates seen in the first wave.
Plus, I agree very much with the Popular Science article regarding short term reinfections (after 1-3 months). Not cheery but reasonable IMO. We have seen many cases of long lasting diseases (months) and some of the infected reinfections could mbe much of the same.
A different matter will be 6-12 months after clearance. We will see.
This made think about an argument i saw days ago here about remarks from Taleb in the sense that the overall protective effect of mask usage at social level is higher that the measured effects for each user. I think he is very much right because mask usage affects two different processes: virus shedding and virus uptake and the net effect will be better than the sum of both. Synergistic effects can be expected.
Plus I don’t see the Popular Science paragraph as cheery. I think it makes a good exercise of reasoning. I would add that given there are many reported cases of long lasting infection (months) some of the so-called re-infections are simply the same infection where the inpatients had only apparently cleared after the first acute episode.
This is talking about short term re-infections, up to 3 months after the first acute cycle. A different matter will be what we see 3-12 months after the first infection. Will people that passed this this spring go to a second round next autumn?
Re: “Further, all the presenters give me the feeling that they are medical scholars, and not academic entrepreneurs, dying to get into the business school, or make money ramping some stock.”
Here here….Especially with “pump and dump” stock moves (notably Moderna), MSM broadcasts seem littered with “medical experts” commenting on vaccine research who have not disclosed their financial relationships with those pharm companies or are auditioning for a high paid position.
I just read about an Israeli physician who was infected twice. I wonder if these are re-infections or if the virus somehow can go dormant for a period?
https://www.jpost.com/health-science/israeli-doctor-reinfected-with-coronavirus-3-months-after-recovering-635550
It’s in the post.
I think this is way more possible than the experts think because:
1. If we take 3 months as a minimum for reinfection (a true reinfection, for the sake of argument, since this appears consistent with minimum timeframe for common cold reinfection and the common cold is the cornavirus with the shortest immunity time period of common coronaviruses) most places in the world ex the US, UK, and Sweden went into rapid containment mode and got infection rates way down via lockdowns, and later contact tracing and quarantines. So it doesn’t appear there are many places that you have three months plus of high levels of community spread.
2. In the US, infection rates started rising in late March, but recall we interrupted that with April lockdowns. The infection is way down in NY. So CA may be the only place with a high-ish level of community infections for 3 months plus. In FL and Texas, infections were low until June.
3. Due to lack of testing, a lot of early and current infections are simply not being diagnosed. And I have heard of people who had symptoms that sounded spot-on for Covid but the tests came back negative (one repeatedly despite long duration of symptoms). If they did indeed have it, I suspect the culprit is poor nose swabbing rather than poor lab processing.
It will always be difficult to say with certainty but we must count on all possibilities. This virus is infecting millions with so many different outcomes. My opinion is that re-infection is a rare event, let’s say about 1-2 month after the first. Long lasting Covid infections have been reported and some of the cases reported as re-infection could be this: new acute phases after apparent clearance. This virus infects a very wide range of cell types and may not always follow lytic cycle in some cell types, progress through direct cell-to-cell contact in remote organs/tissues relative to the initial infection sites. If this occurs for some time, virus particles will not be sheded and remain undetected for some time (PCR-negative several times but still infected). This is common for certain virus that infect cells in the nervous tissue (think Herpes). But of course, short term re-infection cannot be ruled out though in most cases it will be quite difficult after innate and specific immune activation. But immune conditions vary a lot amongst millions of individuals.
Such outcomes, which I deem as rare, are of course important for a particular individual, pretty much like the reported and damaging long lasting infections, but are not that worrying from the epidemiological point of view. IMO the real concern from this point of view would be the frequency of longer term (after 3-6 months) reinfections meaning the immune response wanes too rapidly in a significant part of the population and casting doubts on the efficacy of vaccines.
“But immune conditions vary a lot amongst millions of individuals.”
This is a very important point. When public health officials push for 95% vaccination, it isn’t just because some people can’t get vaccinated (e.g. newborns, immuno-compromised, etc…), but because some people will not retain immunity from the vaccination. For some reason their bodies just don’t respond as expected. With covid it’s like a real massive experiment. We shouldn’t be surprised by odd ball cases because when millions are getting infected even something in the sub 1% likelihood category is a real countable number.
Just a quick comment on masks. Over the last few weeks I have been closely observing mask use when I have to go out and as I am the dedicated shopper (and cook) for the farm with three generations living on it I do get around more than I would like.
The vast majority of masks are the store bought blue pleated “medical” masks. Looking close almost every time you can see in the sides especially at the pleat. Many times you can even see their lips. When they are looking down such as a checker or just someone looking down you can always see down along either side of their nose. Even with metal strip the nose area opens and closes as they talk and the sides open too.
The snood pulled up over the face seems to be pretty good if you can seal the nose channels. I believe that rather than trying to push down the mask into this area a better fix is to put a strip of padding/foam or something there on both sides.
Bottom line most masks are doing very little to “filter out” particulate. But hey, at least they are wearing them right?
I have noticed quite a few mask over the mouth but not the nose. Not really sure where that comes from and while a bit concerning is mostly comical.
In many people the air stream from the nose is downward. It depends on the nose architecture, which varies between ethnic groups.
The Air stream from the mouth is generally more horizontal.
IMHO The most uncomfortable part of the mask is the nose covering.
Some of those not covering the nose might be less able to transmit the disease.
I do not recommend testing this hypothesis.
I have a supply of the blue pleated masks. In order to get a snug fit on the sides, I stapled two pleats together on either side. Works well. I also learned that by first folding the mask in half to get a firm nose pleat it is then easier to shape the top of the mask for a closer fit that doesn’t fog up my glasses. I find the blue masks to be the easiest for breathing, but now that I have been able to fashion a more snug fit, the areas of my face where the mask was resting are always moist by the time I leave the store and remove the mask.
I wish I could say the same, where I am. Mask use has dropped way off. I counted 16 people in the checkout area at one store, only 2 employees and 2 customers had masks on,( not counting myself.)
I left, and went back later when it was slower.
Price gouging on masks is not helping. $14.95/10pack for disposable “blue” masks, only ones I have seen locally for sale.
I have not seen a single medical mask online or local, as all are labeled “non medical” dust mask.
Just spoke to someone who shared that a friend of hers “beat” COVID back in March/April, only to contract it again and recently died. We are in the Bronx, NY. Does anyone know if the CDC or any other institution is gathering data on repeat cases of COVID?
I have read of people being infected only three months after their first infection but what that tells me is that it is possible to be infected perhaps four times a year. I suppose the truth is that as the numbers of people infected increase, that there will be more clarity on this. It could be a resurgence of the virus in people’s bodies but the key to knowing this would be widespread testing which has yet to be prioritized.
A lot has been learned about this virus and how to treat it the past six months leading to a lower death rate among people who have been infected. Ventilators are no longer a first response for example in treatment. But as the subject of re-infection depends on a time component, it may mean that we need a larger database of such cases to find out if this is what the virus is doing.
My own guess is that the antibodies that treat the infection disappear shorty after leaving the body to be vulnerable to a re-infection. The implication then that what is needed is a response from the T-cells that have a ‘memory’ that will play out long term to protect that body if there are further infections. Thus any vaccines will have to use the T-cells to give protection against the virus. Only problem is that this virus is not going anywhere soon so it is only a matter if time that it mutates but as to what form is anyone’s guess.
Dr. Ghandi at 42:28 (slide and comment)
She has heard of NO verified or convincing cases of re-infection.
Could be explained by problems with the testing, as it only shows dna traces, not active virus being shed.
“Not verified”? That sounds like an impossible standard, as if it has to be in a lab setting, not the wild.
There are two cases in Israel, one of which looks like a bona fide reinfection. The second a hospital is denying as a reinfection but it came after an MD came in contact with a Covid-19 patient, having tested negative repeatedly after an initial infection.
Here’s the case that looks more dispositive because the patient was symptomatic, not just testing postive. It was in the post but bears repeating:
https://www.jpost.com/health-science/israeli-doctor-reinfected-with-coronavirus-3-months-after-recovering-635550
I’ve heard of one quite convincing case of probably reinfection – a friend of a friend who is a nursing home attendant. Anecdotally, many people who had mild cases or who have tested positive on antigen tests and who work in medical areas are getting quite careless (my niece, a hospital doctor, was joking recently about having ‘antigen positive parties’).
The problem of course is that with the first wave in particular, there were undoubtedly many false positives and negatives and a generally chaotic approach to saving samples, so ‘verifying’ reinfection to a level of scientific proof would be very difficult.
I always have difficulties when I hear scientists make careless comments on topics like this. Why, for example, should it need to be ‘verified’ that reinfection can take place rather than working on the assumption that it does, unless it can be ‘verified’ that it cannot? Sometimes even the best scientists betray underlying assumptions and bias.
The problem is that verifying this is nearly impossible and saying that “it should be verified” is more rhetorical than practical. In this sense this is careless talk.
But scientifically ,I don’t think is careless to say it should be verified because scientists know that it could be a different case in which virus infection was not readily cleared and resumes into a second acute phase. While the possibility of reinfection cannot be ruled out it is always considered rare due to both innate and specific immune responses. I don’t think this is bias, but making the right questions while counting on re-infections as a given would be a biased assumption because you are ruling out other possibilities.
I agree – my overall point is that since the beginning of this epidemic many experts have started on the basis of certain assumptions, many of which seem to me to have been based on quite light evidence, and without taking account of risk factors (i.e. Talebs point about long tailed risks).
From the very beginning, there seemed to me to be a default assumption that infected people would have some element of immunity. This was always likely of course, but it seemed to me that waiting for ‘proof’ that people could get it twice was the wrong approach. The default assumption should (in my opinion) have been that getting reinfected was a significant risk. If this default had been taken, I think the issue of ‘herd immunity’ would have been taken off the table much more quickly.
I also think that there was a default assumption that this disease was like a flu (rather than, say, like polio), which implied that once cured, people could just get on with their lives. Again, I think this was an assumption with little evidence to back it – it was an approach based on a implied conceptual model, not one based on a deep knowledge of the virus. Had we not made this assumption then from the beginning there could have been more efforts made to monitor patients for long term damage.
I understand your objections: being this a new disease caused by a new virus of which nothing was known we couldn’t think on concepts as herd immunity as a given or something that could be achieved without pain, a lot of pain, in a short time span. I think that very few thought this and the political responses were more political than scientifically based. Even worse, the calls for ‘herd immunity’ were possibly something as simple as political laziness (nothing will stop business as usual), or even worse laziness combined with something more obscure if you don’t mind paying a high toll for doing business as usual. Very much like politicians picking conceptual economic frameworks that haven’t been developed on solid grounds but to give a credible narrative to their political agendas. Some politicians just picked a model that did not get in the way of their agendas.
Then after the disease got us by surprise in most places there were not resources available to do the careful monitoring you are asking for while in others, with relatively few cases, it was just difficult to find and identify those relatively unusual cases except retrospectively. As we are learning, more importance will be given to those but yet the priority is given to the treatment of the severe cases. We are early in the epidemic with yet a lot to learn about this. Such learning requires an effort and we are quite possibly not doing the best of our efforts. But this also requires time, we are talking about developments that take months to be detected and analysed further.
When you say that the call for herd immunity may have been laziness combined with something more obscure, (in the sense of being unknown), I think of the Spanish word “oscuro”, which means dark. It seems a more appropriate word.
In trying to sort out this reinfection problem we are hampered by having to use PCR to detect infection. This test by its very nature is picking up sars CoV 2 viral RNA. It doesn`t tell us if it is picking up viable virus, which in these circumstances is an important point. Then the fact that you need a high bio security lab to actually culture the virus means we can`t, for example, compare the virus someone first tests positive with, with the virus found 2 – 3- 4 months later when the person becomes ill again and tests PCR positive again.
This is a really hard nut to crack
Liked Ignacio`s comparison of politician`s behaviour dealing with the pandemic and same over economic policy choices!
Hey, Ignacio, I see nothing wrong with herd immunity as a concept. Only as strategy.
The concept is perfectly valid, as it describes a situation, rather than prescribing an action.
Seems to be used, now, as a synonym for a policy of “ignore it and let it spread”, but this is not what it is about, at all, right?
I read a few days ago that Johnson was increasing the NHS budget quite significantly to fight Covid-19. I don’t remember the precise numbers and how this measure compares with similar efforts done in other countries but it might be the case he is now having better (though late) reaction than other leaders and possibly he does not have the austerity limits being imposed in some EU countries. I will try to find comparative data on this.
£5bn apparently for an increase in NHS budgeting specifically for COVID-19 https://www.gov.uk/government/news/chancellor-provides-over-14-billion-for-our-nhs-and-vital-public-services
We’re going to have to see how much of that turns into real, front-line benefits — and how much truth there are in the warm words of “public services would get whatever they needed”.
But yes, U.K. government has allocated an additional £300bn fiscal spending for 2020 in response to COVID-19… a figure which mysteriously enough is exactly what the Bank of England announced will be the increase in asset purchases https://www.bankofengland.co.uk/monetary-policy/quantitative-easing
Not, of course, that the Bank of England is monetising the government’s debt issuance. Ooh-noo. Not at all. It’s just pure coincidence!
Thank you!
And, of course, he experienced the disease, which could have made a difference in attitude — what’s worth paying for.
Sorry, I used the word “verified”, not Dr, Ghandi. She said there were no “convincing” cases of reinfection.
If it is common to be re-infected within a few weeks after recovery, I think we would have a lot of reports of it. I would expect there to be a few re-infections of any disease, just because of human variation.
So, yeah, it’s possible, and probably does happen, but it’s not common enough to worry about.
3-6 months afterward is a different story.
Also, would a re-infection necessarily have worse symptoms than the first go-round? If you survived it once, would the sequelae (after-effects) from the second time be worse?
Looks like our Preener in Chief has finally embraced masking as Patriotic, per his latest tweet. Don’t listen to the FailingDishonestMedia, your ‘Favorite President’ has *always* supported masks (where appropriate)! Oceania has always been at war with Eurasia!
….Which he should have done long ago of course. But it’s still a trap for the Etats General. They tend to keep beating him with the same sticks, amping up the rhetoric, never recognizing that the non-TDS majority whose motivations they can’t be arsed to understand has tuned them out.
… Also, most people recognize 20-20 hindsight when they see it, so the hyperbolic OrangeMan Murdered 150,000 People crap starts sounding like, oh, so you’re claiming tha Covid wouldn’t have come here if Hillary had been in charge? or you would have overriden all the (Democratic) states and cities straight away and kept us all at home? etc. Especially with swiss cheese brain Joe getting carried away every time he’s given a mike.
It doesn’t wipe away the big black eye for Trump, since he has in fact done little but whine, deflect and self-justify, but it starts eroding the line that the other buncha jerks have their act together any better.
… I believe that, plus the inevitable unveiling of the Blob’s preferred affirmative action VP takes the country back to its rough 50/50 split by Nov 4. Barring yet another body blow to the nation of course, which is entirely possible in this aptly named Year of the Rat.
> Oh, so you’re claiming tha Covid wouldn’t have come here if Hillary had been in charge? or you would have overriden all the (Democratic) states and cities straight away and kept us all at home?
See Appendix here.
The liberal Democrats frame the COVID-19 debacle as a failure of leadership (when it’s systemic). Unanswered is this question: If Trump had “led,” would Democrat states have followed? I’m guessing that Cuomo and Diblasio’s disastrously slow and feeble initial response would have been no better — and quite possibly worse, out of spite — no matter what Trump did.
And what does leadership matter when the country lacks the operational capability for a functional response? Better public relations about swabs could be better, no question. But still material realities intrude: The swabs must be made. And that we cannot do. For example, suppose Trump had invoked the Defense Production Act and started one or several green field swab plants. What then? Wnere do we get the machinery? We don’t do machine tools anymore, let us remember. And on and on and on.
Oh, absolutely, but there is no systemic change on the menu this year, sorry. Not much ‘call’ for it round here, sir, and anyway, the cat’s eaten it.
If extreme measures are needed to save the economy and keep people from financial ruination, aside from jobs programs addressing such issues as the neglected infrastructure, the more immediate and pressing concern of the pandemic could be addressed by establishing cottage industries throughout the country involved with and related to covid 19. Even contact tracing could potentially become so much more efficient, therefore actually useful. I see it as a way of increasing operational capability for a more functional response and offering people jobs at the same time. Btw, we still have machinists, machine tools and vintage machinery. It’s old school and very “legacy”, but the knowledge exists. Perhaps it’s appropriate to say that the economy needs retooling.
We can speculate all we want on how a hypothetical Clinton administration would’ve responded, or how Democratic governors would’ve responded to a competent a competent approach from the Trump administration. But, none of that happened. Trump’s response has been disastrous, and it sure seems like people would be letting him off the hook by making such impossible to prove claims about something that hasn’t happened.
“we can’t make cotton on a stick” is something i’ve thrown at some of my right wing friends and relations a lot since march or so, when attempting to lead them out of the Free Market Cave, from whence it still looks reasonable to offshore all our productive capacity.
that phrase almost always shuts them right up, and i’m able to then advocate for them to buy seeds and stick them in a closet for the Coming Darkness.
(and yes, i understand it’s a little more complicated than affixing some cotton on a stick…still, it points a pretty big finger at just how far we’ve fallen from the Man on the Moon Days)
Maybe liberal Democrats would have handled Covid-19 the same way Obama handled the Flint water crisis?
Thanks for this, a really interesting video, I learned a lot from it. The ending (last 5 minutes) is particularly informative – it seems that the focus at the beginning of the outbreak on fomites was misguided.
I recall from the very beginning back in January looking at videos from Wuhan where there was a huge focus on face masks, but everyone seemed quite casual about bare hands on surfaces (on public transport, for example). I wonder if this was based on science, or a general cultural belief in China and other Asian countries that aerosols and droplets are far more dangerous than hand to face contact. I really wonder if this divergence between Asian countries and everyone else is based on past experience, or is cultural, or if there is another explanation. Whichever way you look at it, its clear that the reflexive Asian approach was correct. A lot of public health experts (in particular those who have been anti-mask) need ask tough questions as to why this happened – it undoubtedly cost lives.
Wearing a mask discourages you from touching your face, it’s one of the Big Three Benefits of wearing a mask. So, a mask-wearing culture is a little less vulnerable to surface-carried germs.
Wow, I just saw Dr. John Campbell’s most recent covid-19 video and it’s about a new peer reviewed study just published in Nature. The study was around immunity to covid-19 if you had SARS-1 (2002/03 version). Interestingly it also included a control population of people who didn’t have either virus.
Key conclusion…
1) People who had SARS-1, 17 years later, are still showing long memory T-cell immunity.
2) There is a cross-immunity response between SARS-1 and SARS-2 (covid-19).
3) Of very intriguing interest, a significant number of the control group that did not have either SARS virus showed T-cells capable of attacking covid-19!!! They did confirm that this immunity didn’t come from recent exposure to the common cold (another type of coronavirus), but from having been exposed to betacoronavirus. Betacoronavirus is very common in cows, dogs, bats and rodents.
https://www.youtube.com/watch?v=R3_wSU1JnTE
https://www.nature.com/articles/s41586-020-2550-z_reference.pdf
Yeah, SARS CoV-2 is a beta coronavirus. Just so no misunderstanding in terms.
Isn’t it possible these people are catching a different strain of SARS-CoV-2?
There is only one strain from an immunological perspective, so far. SARS-CoV-2 doesn’t mutate that fast.
This sounds like good info, so thanks for posting it. But I’m so confused now I think we might as easily be misguided. For instance, nobody who has kids thinks it is true that kids don’t give you their colds and flus. Parents catch everything their kids bring home. It’s legendary. So it begins to look like panic over the economy when they say optimistic things. I’m sure the jury is still out on corona reinfection and chronic conditions. When it comes to human health there is almost no standard; we are all adapting individually. But one thing is clear: the economy is in danger of dying on the vine. To me that explains why there is some noisy push to put kids back in school and minimize the danger from corona. If kids don’t go back to school parents can’t go back to work. Etc. Another unknown is, What wave are we in? Still the first one which we failed to quarantine? Or the second one which is predicted to be worse? The Spanish Flu had three distinct waves before it fizzled out. And in spite of all the hype about a vaccine, there are still a lot of people who think a vaccine isn’t even possible. And “herd immunity” has been debunked not because some people do develop antibodies, but because it is so gruesome achieving it for an immunity threshold. So where does all this leave us? Wherever. Just wear your mask. One thing I’d like to know is what is the best UV lamp to buy for the coming winter season – anybody got suggestions?
for Susan:
not an expert on this but I heard about a far UV C wavelength a while back that is safe whereas what has been on offer up to now is a dangerous wavelength see below:
“…….. rare UV-C is the ultraviolet light of choice for purifying air and water and for inactivating microbes. These can be generated only via human-made processes.
UV-C light in the 260 — 285 nm range most relevant for current disinfection technologies is also harmful to human skin, so for now it is mostly used in applications where no one is present at the time of disinfection,” Zollner said. In fact, the World Health Organization warns against using ultraviolet disinfection lamps to sanitize hands or other areas of the skin — even brief exposure to UV-C light can cause burns and eye damage”
https://www.sciencedaily.com/releases/2020/04/200414173251.htm
BUT there seems to be another UV C wavelength, far UV C, that achieves the same without doing any damage at all to human tissue and I found a link explaining it. see below:
https://www.cuimc.columbia.edu/news/far-uvc-light-safely-kills-airborne-coronaviruses
Sorry though, no idea where you can get the lamps or if they cost a lot being new!!
hope that helps…..
I had the links, but can’t find at the moment, for the far UV-C lamps.
They were very expensive, and required special power supplies. Only one company I found making them, and not readily available to the public.
These are not consumer products. They are being tried experimentally in medical facilities,etc.but are not yet proven safe for any normal routine use.
UV-C lamps are dangerous unless you are completely shielded from exposure, and this limits any possible uses in the home. You could maybe disinfect some small items, but getting a good exposure all around the item would be difficult without multiple lamps.
Heat/alcohol/bleach seem to be the go-to, for now.
Right. Well-shielded UV mounted inside a fan or HVAC is the way to go.
Thanks for the info SKM – I’ll go surfing and see what I can find.
Remember that microbe.tv and the TwiV (this week in virology) podcasts has regular information updates from scientists, clinicians, and includes links to papers and such. Also ‘immune’ and other podcasts there. I recommend especially you listen to TWiV 640, about testing.
yes TWIV 640 is a must listen too for the brilliant idea someone has had re testing – a game changer “Test sensitivity is secondary to frequency and
turnaround time for COVID-19 surveillance” Larremor et al. Sounds like a game changer, if rolled out could mean real time testing/results for everyone (workplace, schools, flying etc)
A 50 min video by Chris Martenson which, I think, makes a convincing case for reinfection:
https://www.youtube.com/watch?v=qhyEBIpaIaM
Thank you so much for this, Lambert. You’re a treasure.
IMO, this is huge and isn’t getting the attention it deserves.
“Nearly two weeks later, she took an oral and nasal swab test. The oral test came back negative, but the nasal came back positive.”
A difficulty with most tests is that they pick up fragments of the viral RNA, which may mean infectious virus or just litter from an infection. They are not like plaque assays which measure growth of replicating virus. Serology tests can measure antibodies, but just doesn’t tell if replicating, or transmissible, virus is present. The key for the public health is testing for transmission, which is not the same issue for testing to determine what to do with the prospective patient.
On reinfection:
While looking at scientific literature on vaccines (I am resorting to reviews as there are mountains of publications) i have come to a hypothesis for re-infections which should be somehow tested: it could be the case that such re-infections, or a subset of them, could be true reinfections due to increased susceptibility via ADE (Antibody Dependent Enhancement of the disease).
ADE has already been described in some many instances including humans and animal models. It has been frequently seen in infections by Filovirus (Dengue, Tika) but it is not exclusive for those. It has been seen in a feline disease caused by Coronavirus and also in vaccination trials against SARS1.0 in animal models. ADE may have different outcomes: it can result in more severe disease and/or it can result in frequent infections and reinfections. This is why I believe this could explain those re-infections in short times.
To test this hypothesis full immunological analyses of plasma from the affected individuals should be done: analysis of antibody titres, virus neutralization with convalescent plasma, in vitro ADE assays in cellular cultures etc… It should also be reported to the WHO, vaccine developers etc. and it should be tried to determine what is the overall frequency of this phenomenon and if it can be anticipated by serological analysis to be done in vaccine trials. The severity of such possible re-infection processes should be carefully addressed.
ADE is being addressed in Covid vaccine trials in both the preclinical and clinical phases, but research in re-infections to confirm or rule out a role for ADE in Covid infected humans should help to analyse this risk, decide extra studies and select better candidates.
Thanks for this – it really is such a complex topic – I am more and more sceptical of all those media reports about ‘successful’ vaccine products. We may get lucky, but I doubt if we will see a true universal vaccine for a few years.
I’d be interested in your opinion on whether it would be better to focus on a more generalised vaccine that would simply boost our immune systems rather than specifically fight Coronavirus? There seems quite a lot of information that existing vaccines can be protective. Maybe if they focused on boosting these and giving everyone in the population a booster shot for TB/Mumps/etc., they could act, not to protect everyone, but to reduce the pool of available susceptible people to reduce R0 below 1?
You are asking on the BCG vaccine that boosts (this has been reasonably well studied) the innate immune system (innate vs. adaptive or specific humoral and cellular response). It is indeed all important to check how this works preventing and/or ameliorating Covid 19 outcomes.
Coronavirus have developed ways to evade the innate immune response which are based on cellular systems that detect viral infections in the initially infected cells and rapidly respond via type I IFN signals preventing viral replication in the initially infected cells. CoVs interfere with some steps of this system and it is suspected that the long incubation period observed for Coronavirus has to do with this: it is the initial inflammatory response what produces the first symptoms upon infection. So, our body may do not detect CoV infection until the first infected cells die releasing ‘tons’ of viral particles and resulting in further virus spread plus more severe outcomes. The specific immune response is also delayed.
Upon BCG vaccination, the innate immune system is boosted through epigenetic changes in the DNA and this can protect against a variety of infections. After BCG vaccination, our innate system becomes ‘trained’ and so it could be more difficult for CoVs to evade this. I hypothesize that the efficacy of such vaccine would be lower than vaccines specific against CoV but the results now being tested could be a significant reduction of number of infected and a reduction in the severity of the disease. This is being tested by an Australian University if I recall correctly and is now first in the list of WHO vaccine candidates. The reason for this is that we can count on good safety with this vaccine.
My opinion is that this can be important and it can really be the first candidate available that could help a lot even if the efficacy is well below the standards with specific vaccines.