Yves here. This post confirms what IM Doc has been saying for some time. For instance, via e-mail in April:
As a young child, I saw my father [a public health officer] struggle through the Swine Flu of 1976 and the vaccine debacle that accompanied that era.
As I grew older, and especially once I entered medicine, he had several heart-to-heart talks with me about a career in Medicine and by extension public health. I can summarize what he told me in two large thrusts. 1) Integrity, truth, and honesty is EVERYTHING in public pealth. Once squandered, it will never return. 2) Public health is 10% science and 90% psychology. Do not ever forget that. You will get nowhere by screaming SCIENCE SCIENCE SCIENCE and you will certainly get nowhere by flashing credentials. And you must have an acute awareness of panic, fear and anxiety. They change everything and your response must always take that into account.
Here, initial Covid failures and the elite pretense that they could just carry on as if that were a thing of the past, as opposed to admit to the errors and discuss how they planned to do better going forward, has exacted a price in terms of trust, as this post below explains.
By Geraldine Blanchard-Rohner, Senior Pediatrician and Immunologist, University Hospital Geneva; Bruno Caprettini,SNF Ambizione Fellow, Department of Economics, University of Zurich; Dominic Rohner, Professor of Economics, University of Lausanne; CEPR Research Fellow; and Hans-Joachim Voth, UBS Professor of Macroeconomics and Financial Markets, Department of Economics, Zurich University. Originally published at VoxEU
As COVID-19 vaccination programmes accelerate across the industrialised world, vaccination hesitancy is rapidly emerging as a key challenge. This column explores the relationship between pre-pandemic intensive care unit capacity and attitudes towards the COVID-19 vaccine in the UK. Despite widespread pre-pandemic scepticism about vaccines in general, willingness to become vaccinated against COVID-19 overall was strikingly high, even amongst those who rejected vaccines before the pandemic. The results point to a surprising synergy: where the emergency care systems of public healthcare providers were less strained during the early days of the COVID-19 epidemic, vaccination hesitancy is systematically less today.
Since February 2020, the COVID-19 pandemic has cost millions of lives and has affected almost every aspect of economic, social, and cultural life – from stock markets to inflation, schooling, inequality, and the gender division of labour, to name but a few (Yeyati and Filippini 2021, Burgess and Sievertsen 2020, Baldwin and Weder di Mauro 2020, Capelle-Blancard and Desroziers 2020, Sevilla and Smith 2020). Infection rates surged around the globe, and medical systems came under increasing strain.
In recent months, vaccination programmes have accelerated across the industrialised world. With supply problems increasingly solved, vaccination hesitancy is rapidly emerging as a key challenge on the path to herd immunity (Troiano and Nardi 2021, Dror et al. 2020). Given the high infectiousness of new variants, vaccine take-up amongst adults will have to reach particularly high levels for COVID-19 to be brought under control.
Our new study offers novel lessons about the drivers of vaccine hesitancy (Blanchard-Rohner et al. 2021). A previously overlooked factor can be crucial, namely, the efficiency and success of public healthcare provision during the pandemic. When the pandemic first broke out, intensive care units (ICUs) in many countries and regions were quickly overwhelmed, resulting in high mortality rates.
Using newly collected survey data from the UK, we show that success in providing emergency care during the dramatic initial phase of the pandemic is a powerful predictor of people’s readiness to receive the COVID-19 vaccine. Where the NHS was quickly overwhelmed, with overcrowded ICUs and high COVID-19 fatality rates, the willingness to become vaccinated is markedly lower.
Our findings suggest that there is an important, neglected synergy between an effective healthcare response in the early phases of a pandemic and the public’s trust and willingness to use novel treatments like the new COVID-19 vaccines.
We conducted two waves of interviews about vaccination attitudes in a nationally representative sample in the UK – in the autumn of 2019, before the pandemic; and in April 2020, during the first wave. We interviewed the same respondents, which allowed us to track changes in attitudes over time. These changes we then correlate with the quality and effectiveness of emergency care in different areas of the UK. In total, we had 1,653 respondents in the first wave, of which 1,194 participated in the second wave.
Respondents included a sizeable share of vaccine ‘hesitants’ and respondents who outright reject vaccinations – participants who in the fall of 2009 had declared that it was better for children not to receive vaccines, or that vaccines cause severe adverse effects including autism. We estimate that 12% of respondents reject vaccinations altogether and another 36% are sceptical. Only 52% of participants were strongly positive about the effects of vaccines in general prior to the pandemic.
Despite this widespread vaccination scepticism, willingness to become vaccinated against COVID-19 overall was strikingly high – some 85% of study participants said that they were definitely or probably willing to become vaccinated. Remarkably, even amongst those who reject vaccines or are hesitant, 55–81% are willing to participate in COVID-19 vaccinations (Figure 1).
Figure 1 COVID-19 vaccine acceptance and general vaccine attitudes
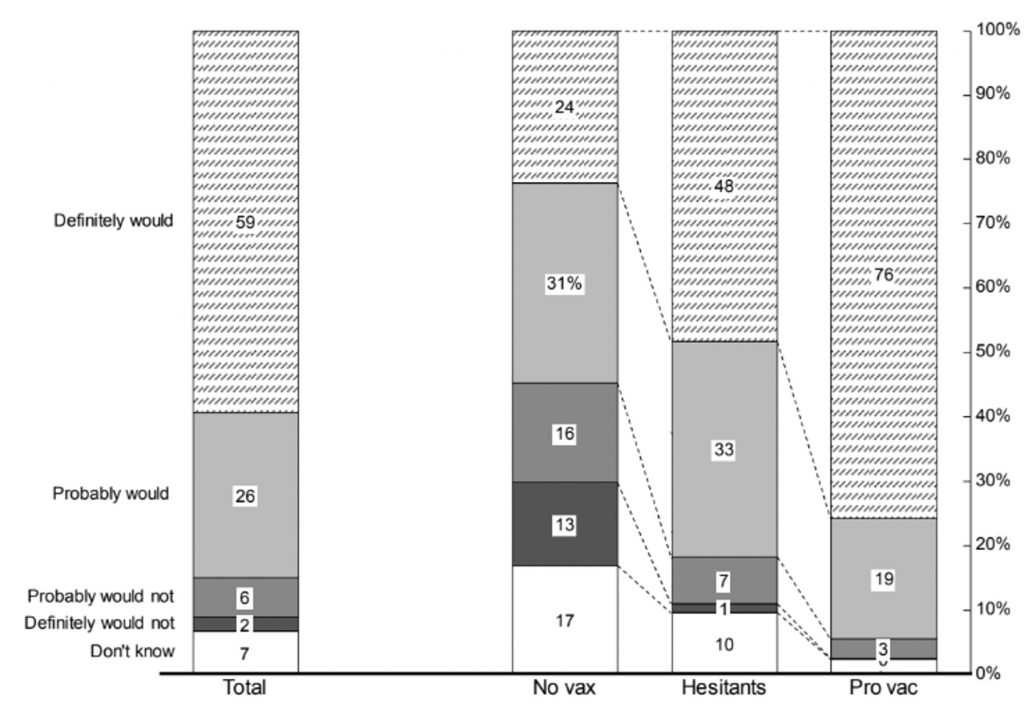
Source: Blanchard-Rohner et al. (2021)
Notes: The figure shows responses to the question: “If a vaccine against COVID-19 became available for everyone tomorrow, do you think you would or would not get vaccinated?” The bar on the left reports the breakdown for all respondents of the April 2020 survey (N = 1194). The other 3 columns report the breakdown for three categories of respondents: “no vax” (N = 148), “hesitants” (N = 431) and “pro vac” (N = 615). We assign respondents to one of these categories using ther answers to the question on general vaccination attitudes. See Section S.2 in the Supplementary Materials for details on the construction of these categories.
Several interpretations of this fact are possible. Vaccination sceptics may feel that most diseases against which vaccines are routinely used are not terribly harmful; faced with a potentially deadly illness, they change their mind. Alternatively, sceptics may have updated their beliefs in the face of the COVID-19 pandemic, with 24/7 media coverage of the disease, its consequences, and the need for a vaccine.
Our second main finding involves the role of public health provision. Before the arrival of vaccines, the availability of ICU capacity was a key determinant of mortality – where intensive care beds were missing, death rates spiked. We exploit the fact that various areas of England had different pre-COVID-19 levels of ICU coverage. This, in turn, meant that NHS hospitals in some areas ‘ran out of road’ much faster than others once the pandemic hit.
When we examine simple correlations, we find that low ICU capacity during the first wave of the pandemic is associated with lower vaccination willingness. This is not a result of pre-existing attitudes but a direct consequence of how vaccination hesitancy changed during the pandemic.
Panel A of Figure 2 plots vaccine hesitancy against ICU occupancy rates in February 2020, before the UK saw its first major spike in cases. The higher pre-crisis capacity usage, the greater hesitancy was by April 2020. In other words, where exogenous variation in ICU demand pre-epidemic had reduced spare capacity in ICU units, the pandemic struck harder.
Figure 2 ICU availability, perceived risk and unwillingness to get vaccinated against COVID-19
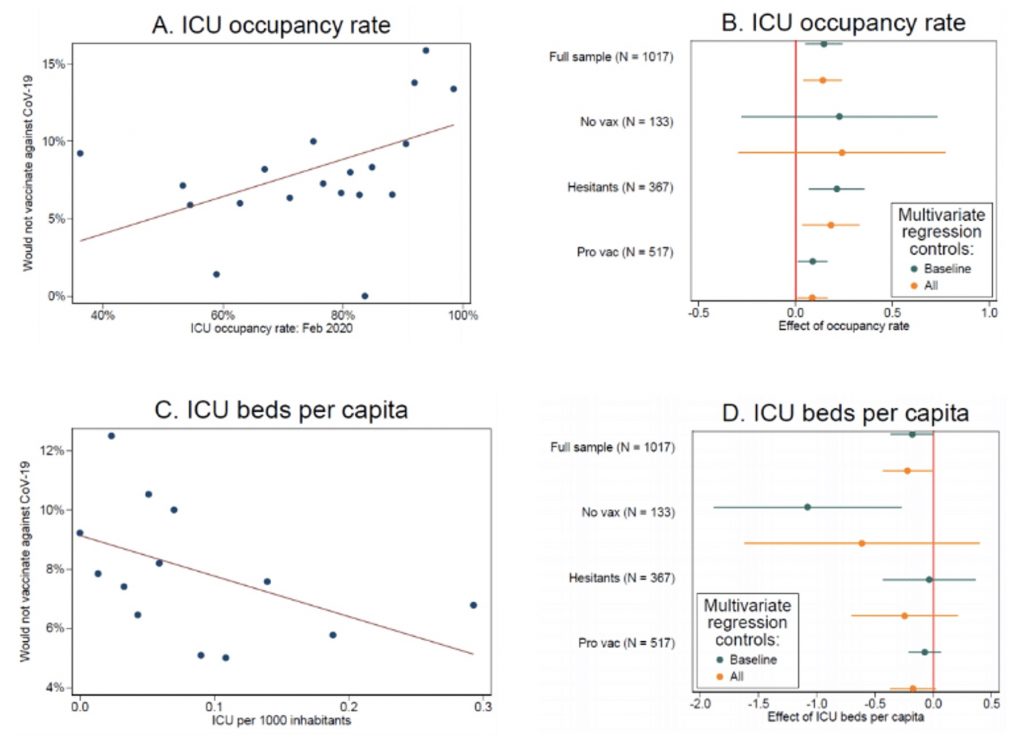
Source: Blanchard-Rohner et al. (2021)
This failure to provide effective support was not a result of structural under-provision in certain areas. No such pattern is visible if we use, say, ICU occupancy half a year earlier (October 2019), strengthening the case for a causal interpretation of our finding. Figure 3 gives an impression of the variation in ICU occupancy across Britain on the eve of the pandemic’s first wave, in February 2020.
Panel B of Figure 2 shows the same exercise for different groups, and after controlling for observables. We find positive effects throughout. The analogous pattern is visible if we use the number of ICU beds per 1,000 inhabitants as an indicator of public health resources.
Figure 3 Variation in ICU occupation across Britain in February 2020
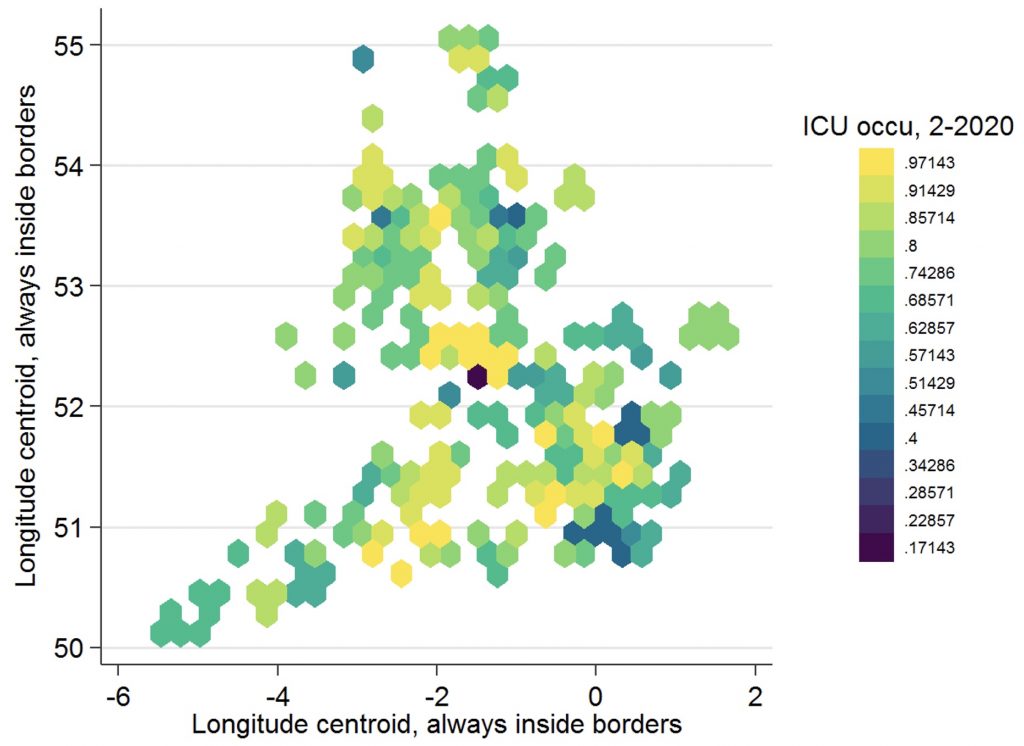
Source: Using data from Blanchard-Rohner et al. (2021).
Policy Implications
At first pass, many observers could think that public health resources like ICU capacity and vaccination campaigns are substitutes – countries with high capacity to deal with severe cases might be able to cope with lower rates of vaccination take-up. However, our results point to a surprising synergy: where the emergency care systems of public healthcare providers were less strained during the early days of the COVID-19 epidemic, vaccination hesitancy is systematically less today.
While generally high rates of support for vaccination make it more likely that herd immunity can be reached, our findings suggest that generous provision of spare emergency capacity can generate additional benefits, in the form of the public’s greater willingness to become vaccinated.
See original post for references


Back in the 90’s I did some research on the public communication of risk, especially when dealing with scientific uncertainty. The key thing, known even back then, is that while people may not understand the science, they do know when they are being lied to, and in particularly know when they are being patronised. Oddly enough, it seems the more educated you are, the less likely you are to recognise educated BS when its been fed to you, perhaps because part of a university training is to learn not to question those with more impressive looking degrees than you.
Its also worth pointing out that many ‘experts’ fall deeply into a number of cognitive biases, while the general public tend to have learned to use simple heuristics such as ‘assume Homer Simpson is at the controls’. In many cases, the latter assumption has been proven to be more correct. I’ve lost count the number of times I’ve seen engineers and scientists essentially construct a tightly controllable series of ‘tests’ for safety or accuracy, and then, without any justification, extrapolate their conclusion far more widely than can be justified. In simple terms: ‘my lab mice didn’t show any signs of cancer, therefore this chemical is safe’.
The first warning sign of this in Covid for me was when WHO and a number of public health bodies started insisting that there was no need to curtail travel. This amazed me, as I didn’t realise a virus could grow wings. When I did a quick search on the WHO website they quoted a number of studies in Africa, mostly involving Ebola. Given everything we knew about infectious disease from Roman times is that they travel on the same routes humans do (such as the Russian Flu of 1898 following the newly built cross-continental rail lines), this just seemed bizarre. For me this was a warning sign that many scientific authorities were more interested in managing the news in the way they thought best, rather than issuing clear, untainted advice. Sadly, it wasn’t the last example of this.
If there is one lesson to be learned, its that whatever scientific bodies do when communicating risk or hazard, they should never fall back on ‘noble lies’, or oversimplify. If you are direct and honest, particularly with those things you don’t know, most people will understand. As Noam Chomsky once pointed out, there are few things more complicated than the rules of American Football – if a gas station attendant can talk intelligently about football rosters, then he can understand most of what anyone should need to know about high level decision making.
You write what I’ve been thinking. Thank you.
Travel continuance + we don’t need no stinkin’ masks = ZERO chance for effective public health measures in the U.S. Any remnants of faith in our criminal for-profit health care establishment neatly destroyed with a one-two punch. Heckuva job, Tony!
Heuristics have been proven to be a remarkably efficient means of avoiding negative outcomes in organisational studies. I returned to academia to complete a Master’s this year, and am taken aback by how frequently specific dogmas are reinforced (for example, barely a day has gone by without a professor repeating the ‘Digitization is efficiency, and efficiency is desireable’ dogma) in a wide variety of subjects. I have to conclude that university educated individuals will typically accept the official narrative as they have been taught to accept the universal backing on which the official argument is built.
The backing is not necessarily strong under closer inspection, leading to the tensions when not everyone is reading from the same hymn sheet
I think I fall somewhere in the middle. Teach the full rules (recognising PhutoniumKun’s point that humans can understand remarkably complex phenomena – with the exception of the offside rule in football). However, recognise that the best of us will lose the ability to implement these rules “on the fly” later in life – I can’t do a quick Bayesian statistical calculation given sensitivity and specificity of a test anymore – so a heuristic is useful.
In short, don’t “just” teach heuristics. If people learn the “proper stuff” early on, then they won’t be suspicious of using a heurstic later in life when they can no longer do the “proper way”.
Worth repeating: Fauci lied about masks, because there weren’t enough PPE to go around.
Now, how can we trust him?
For apologists who say “ah but health professionals have priority” remember that he DIDN’T start a series on how-to-make-your-own-mask. Nope, he showed that CDC senior management simply doesn’t care about the people.
Exactly.
IMHO, the home page of every government website should have offered a make-your-own-mask video and a pattern that people could print out and use.
Oh, and how about the information we all need for keeping ourselves healthy? Thanks to the suggestions of the Naked Capitalism commentariat, I have been following this protocol:
https://covid19criticalcare.com/covid-19-protocols/i-mask-plus-protocol/
Meanwhile, the mainstream media outlets have been eerily quiet on this topic.
an aside: latest tewet from flccc:
“There seems to be a mighty attempt to throttle this live program today at Noon ET.”
https://twitter.com/Covid19Critical/status/1399707000125153290
Which begs the question: If a previously highly regarded and well credentialled official like Fauci was willing to risk his reputation and lie to cover CDC or White House derrieres, what sort of pressures was he under? And from whom?
In my country the failures have been predominantly by the political masters:
1. Vaccine access deals inadequate and compromised by a desire to work within local technological capacities.
2. Hopelessly slow vaccine rollout.
3. Woeful vaccine advocacy program.
4. Stubborn refusal to accept the need for new, purpose built quarantine facilities for Australians returning from overseas. Instead they have relied on persisting with the stopgap policy of hotel quarantine, failures of which have resulted in most of our Covid 19 deaths and several economically damaging lockdowns. And thousands of Australians stranded in high Covid19 risk countries like India, some of whom have died as a result.
5. Utter incompetence on several levels in preventing Covid19 infections in Aged Care facilities . Hundreds have died as a result. Looking at you Richard Colbeck.
Hi Tony
I agree the pollies’ record here is not good (though markedly better than most places I guess) but for me that is to be expected. The media too are guilty (as usual) of both censorship and propaganda in the service of the establishment line.
It is the all-in approach of the medical science and public health authorities that bothers me more. I work in that sector and have found quite astonishing ignorance of the sorts of things discussed her daily. Ignorance on the part of health professionals of even the existence of Ivermectin for example, let alone its efficacy. The pooh-poohing of aerosols. The strident advocacy of vaccines. The snide little asides about naysayers and the ‘negligible’ risk of vaccination. The move in 12 months from ‘this is fine, no more dangerous than the normal flu’ to ‘vaccinate now, this is a life and death emergency and it is your duty…’
I am not sure whether Fauci lied or obfuscated ‘to cover CDC or White House derrieres’.. that may be part of it, but I wonder if his words and actions (and indeed inactions) are partly driven not to prevent a particular outcome, but to help ensure one.
I agree Fauci and the big mask lie has caused immense harm. I think he is typical of Washington type elites. He will always assume he is the smartest in room and knows better what is good for everyone. I really do not believe anything these people tell us.
I have family members that will not get the vaccine for fear that it is dangerous. My husband and I got the j and j vaccine. I have been uncomfortable from the beginning about the MNRA vaccine. I had finally convinced my family members to take the J and J vaccine. It is no where to be found now in early June. Several different states where they live and only Phizer or Moderna is offered. I think more people would be willing to take that one, but it seemed to me that DC must have a lot of stock in those 2 big Pharma companies. They have pushed these from the beginning.
Part of a university training is to learn not to question those with more impressive looking degrees than you.
That explains much. I always asked questions of Power. The powerful do not like to be embarrassed.
As for Dr Fauchi, I have never heard so many words and received so little meaning. At first it was amusing, in the end the records breaking obfuscation became obvious.
Experts are generally not free to be honest in what they say or even in what they do. The 1987 book about AIDS, “And the Band Played On,” reminded me that AIDS was not sexually transmitted in the beginning. It was transmitted by doctors (experts) in central Africa by reusing hypodermic syringes. Of course they knew this practice was unsafe, but they were not free to practice medicine in a sensible way. I wonder if doctors are still reusing needles in Congo.
I thing the history of AIDS has been updated since 1987. British Medical Journal, “The early spread and epidemic ignition of HIV-1 in human populations” (2014):
I assume the relation between “transport networks” and sex work is clear. Shilts got Patient Zero wrong too….
“Where the NHS was quickly overwhelmed, with overcrowded ICUs and high COVID-19 fatality rates, the willingness to become vaccinated is markedly lower.”
I could argue that the opposite should be observed – if you see COVID overwhelming things, you’d be more likely to get vaccinated. EVERYTHING about this study either is counter-intuitive or displays a breathtaking ignorance of the likelihood function of the multinominal (logistic) function. People who are unsure typically display a distribution of responses that are much closer to 1/n where n is the number of response categories. People who don’t understand vaccination and are anti-vax are extreme examples of this. THey are overwhelmed with data (much of it wrong or from bad sources). The variance of their responses on the latent “scale of vaccine positivity” is larger, leading to less skewed frequencies. Proved in 1985 and already used by McFadden in his “Nobel” winning prediction of BART demand (analysis done yonks before). It is really disheartening to keep seeing such papers get published. It reflects silo-isation of academia – nobody understands math anymore and how logit/probit models work.
I could write a paper based on the data here that shows that ICU overload leads to vaccination increase, that knowledge of vaccination leads to improved rates of COVID vaccination. Indeed, lets look at the REVEALED preference data as of today. Almost 75% of all adults in the UK have been vaccinated. Even I didn’t expect that target to be hit so soon. Garbage study.
Yes, this is me to a “T”. A lot of my pre-existing conditions that have come up as things that cause problems with people who have had the mRNA vaccines. I pay attention, because I have to. I live alone. No family to take care of me. I am 66, I want to remain independent and I take care of myself in order to keep being able to do that as long as possible. I can isolate, mask, and don’t mind this. I am waiting for an approved inactivated covid vaccine. Not an emergency mRNA vaccine.
There may never be one. Most vaccines will be mRNA-based from now on. It’s the “holy grail of vaccines”. They have been working on this for 20+ years, they finally got the process to work, they are going to use it going forward.
A Danish vaccine is being developed based on a synthetic virus by Bavarian Nordic and some company called “AdaptVac” (Bavarian will be doing the packaging). That’s the closest you will get, I think.
The “Synthetic Virus” concept sounds a lot like the beginning of a Michael Crichton novel, but, what do I know?
All of the “dead virus” kinds of vaccines use a different virus than corona, adenovirus, I think.
I have seen that these vaccines are in trials–one example
https://www.bloomberg.com/news/articles/2021-04-29/a-french-biotech-says-inactivated-vaccines-are-the-way-to-fight-covid-variants
Of course in the U.S. these trials never come up or are pooh-poohed, because not U.S. companies.
I am not convinced the research article is particularly original. The data reflect the neighborhood race and class effects that durably recreate social injustice and inequities across a range of biological and social risks; it is an enduring association. You’d have to govern very differently to get a different, more equitable research association.
Public health is basically a captive of goverance and we will inevitably get the quality of our governance. Sure public health does surveillance and research and risk assessment/mitigation, but much of that is constricted by governing laws and boards of health. Many public health professionals have been constrained by limiting laws from studying gun violence, lead exposure, and much more. Often public health emergency management suppresses dissenting opinions to achieve a public, population action and this role is taken by the rare powerful persons in the profession who are right-hand men/women of governors, not your rank and file, who have to execute actions.
During covid-19, the leadership message often changed to achieve coercive and time-sensitive goals, including from (a) preserving scarce PPE and tests at time one, to (b) encourage wide testing and use of PPE to lower the percent positive rates at time two, to (“c”) selectively distribute scarce vaccines to the elite and aged at time three, and now (d) incentivizing doubting people to get the vaccine through lottery prizes at time four. In one sense, we’ve been getting pretty transparent messages for actions. Of course they are not flattering appeals to higher reason or anything much more than the desire of raw governance for an outcome. It’s the warfare powers mentality way of being addressed that we do not like. Who would?
Considering the political and educational polarities and misunderstandings across the country, I can believe the messages were reasonably vetted by people who do not mean to kill us, but save us. It’s just they don’t trust us any more than we trust them — with reason (we still have a quarter or more of the country trying to violently overthrow the 2020 presidential election b/c they are outraged by democracy.)
We are basically trying to choke down sugar-coated orders with dignity. Even many public health professionals have a gripe, having been suppressed, attacked and blamed for decisions and failures beyond their scope of influence, for Dr. Fauci is at the tippy top of the goverance structure; he’s not your typical public health worker.
Public health has been a troubled public good for many, many years. As many other infrastructures in the country have also been troubled public goods. The root cause is our goveranance, which is real hurky-jerky.
Well, the governed are just as “hurky-jerky”. I recall the election of a reknown body-builder becoming governor of California with less than a majority vote; a WWE ‘rassler” becoming the governor of Minnesota(?); and a “reality tv” character becoming President of the US.
It seems our “democracy” has done little to trend toward competence. Who’s fault is that?
I’m in general agreement with the broader thrust of your comment.
Jerry Brown was on ‘roids’ and pumped?.. Did not know that…
The Arnold was placed in office by the same criminals who funded the also crime spree known as Enron.
The Trumpster became Prez because he claimed to be an outsider, like many before him, and also because his opponent stood for perpetual war, Wall Street favors and said no way in he ll you’ll EVER get Single Payer.
Will defer to Jessie and his ‘you betcha crowd.
The people know there is no choice, the pick what they see as ‘lesser evil
Wasn’t there a listless Hollywood actor that co-starred with a chimpanzee and became the the most patriotic president ever?
I am not sure what to make of this post. The relation between “ICU availability, perceived risk and unwillingness to get vaccinated against COVID-19” seems strange and the explanation offered in the post is unconvincing. I cannot imagine someone following ICU availability to assess risk in deciding whether to get vaccinated.
My own vaccination hesitancy reflects my general mistrust of Big Pharma based on the many cases where money-to-be-made trumped other issues and caused great harm. There is too much money-to-be-made through mRNA vaccines, and too much of that money appears to have greased the wheels at the FDA. Public health policy in the US and statements about the Corona pandemic appear driven by motives other than concern for public health. Much of the research literature appears to serve interests other than Science. The Media spread confusion and misinformation. These factors and others lie at the heart of my vaccination hesitancy, and I never once checked into the availability of ICU beds.
We are far along in a de facto phase III trial of the EUA approved vaccines. But there does not appear to be more than limited collection of small sets of carefully selected data used to demonstrate that the vaccines are safe and effective. That combined with the anecdotes about harmful side effects reported in the NC comments heightens my mistrust. As far as I know, it remains an open question whether the vaccines are effective against the Corona variants; an open question whether vaccines might allow Corona infection but reduce symptoms allowing the spread of the Corona virus by the vaccinated. The lack of follow up this late in the mass vaccinations using the mRNA vaccines greatly increases my mistrust of them.
However, I am seriously considering getting a single dose of vaccine because of what I perceive as a significantly increased risk in even the extremely limited ventures I make to pick up groceries and things I cannot get delivered to my door. I directly attribute the increased risk to the recent Public Health policy pretending the US has beat the Corona flu and approaches some mythic ‘herd immunity’. For now, the Corona virus does not appear to be as variable, durable, or as easily transmitted as the Hoof and Mouth disease virus. Even so, it might be interesting to check on what ‘herd immunity’ there is for Hoof and Mouth disease.
Hmmm. Hoof and mouth disease in humans (not cloven-hoofed animals) is a, non-fatal, minor disease; well studied. Covid-19 is 10 to 20 times more fatal than the annual flu; more so for folks with co-morbidities.
I have no problem with folks who mistrust the mRNA Covid vaccine, as long as they restrict their contact with the herd; or wear an N95 mask when out in public.
I have no problem with folks who mistrust the mRNA Covid vaccine, as long as they restrict their contact with the herd; or wear an N95 mask when out in public. juno mas
Except an unvented N95 is, I’ve read, at most 90% effective at protecting others and at the expense of compromising protection for the wearer – an unreasonable demand, imo.
Instead, those who are concerned about catching Covid should wear a VENTED N95 mask to maximize their own protection (but with NO protection for others) and cease being concerned about whether others are masked or not. (Ideally, perhaps, everyone should wear a VENTED N95 in public to optimally protect (only!) themselves but that’s their business and not ours, imnsho).
I guess I need to clarify my reference to Hoof and Mouth disease. I was referring to the disease in cloven-hoofed animals, not in humans. The idea of herd immunity makes little sense for Hoof and Mouth disease. It is caused by a highly contagious RNA virus that rapidly evolves new variant forms. Some infected animals remain asymptomatic carriers. They do not appear to have disease, they shed substantial amounts of virus in nasal secretions and saliva, so they are able to transmit the Hoof and Mouth virus to other animals. Vaccinated animals can become carriers. A vaccine for one variant category of the virus may not protect against other variants. Vaccination only provides temporary immunity that lasts from months to years. A rancher who relies on ‘herd immunity’ and vaccinations to protect his herd while bringing in animals from other herds might have some unhappy and expensive problems.
Much as I appreciate your tolerance for those who mistrust mRNA vaccines, I can only wonder how much you trust mRNA vaccines. If you trust the mRNA vaccines so much, is your desire that I restrict contact with the herd or wear an N95 mask in public due to concern for my health or concern for your own health in case you might be a member of the unlucky 6% who aren’t protected by the vaccine? In either case, I hope you will be comforted knowing I intend to restrict contact with the herd and wear an N95 mask in public whether I get vaccinated or not.
New York City, which was an ICU train wreck, is undervaccinated.
https://www.nytimes.com/2021/05/06/nyregion/coronavirus-nyc-vaccines.html
They blame it on “disparities” but those same “disparities” are why blacks and Hispanics were hit harder than whites.
In the South, as I have mentioned, all of our Certified Nursing Aides, who are also black, are very vaccine hesitant. Is it memories of Tuskegee? The fact that their relatives generally had disadvantaged access to care when Covid was bad here, and therefore saw MDs late and therefore had worse outcomes? I know at least one part is they know people personally who have had bad reactions (my sense is not train wreck level bad, like dangerous clots, just too sick to work for a day or two) and salaried people are clueless that missing a day or two of work for an hourly person is a train wreck (it can destroy precarious finances and even result in loss of job).
I know little of NYC demographics, so a question. How much of middle-class, i.e. not poor, but still using standard healthcare is actually living (as opposed to working) in NYC?
I’m asking because I could see a scenario where deprived areas = less ICU beds, so the question of casuality would be not ICU, but quality/accessibility of care in general. That’s my main beef with the study. It found a variable, but I don’t think it’s actually an independent one, and I don’t see any attempt to look at it.
For example, the UK has in general way less ICU beds than Europe, yet it seems to have a higher vaccination acceptance rate.
Also, London has a much higher ICU rate per capita than east of England (about four times), yet has much lower (real) vaccination rates. Yes, they may be more “vaccine hesitant”, but they STILL get vaccinated more than the supposedly vaccine-eager Londoners.
Could it be because it goes back to the trust IM Doc talks about? That London has a large transitory population where few people have a GM they know for years, as opposed to other parts of the country, where people might have build some trust with their GM, so if (s)he recommendes vaccination, it overrules the hesistancy?
.
I wish I could upvote this multiple times
Many sites are rife with this cluelessness whenever anything COVID related comes up–then again these are often the same people who don’t understand why everyone can’t just go out and get a job that has gold-plated health insurance or how many people don’t have paid sick leave. Mention things like “on call” scheduling and they think you came from another planet.
I have read numerous articles about how great vaccines are, etc. I have also heard ad nauseum the government/corporate/MSM propaganda generated promoting their use.
I have yet to see or hear any public official/expert/pro vaxxer explain why I should take a product from a criminal organization such as AZ/Pfizer/J&J. The omission of this fact is glaring and very telling about the manufacturers and their products and their advocates/apologists.
Big Pharma Crime Fact Check:
https://www.corp-research.org/pfizer
The word “criminal” is used only once here and that by another poster!
So, personally, my eye is on the unaddressed Elephant in the Room more than anything else.
It’s been incredible to see so many news sites with article headlines about 1) J&J settling massive lawsuits re: their role in the opioid epidemic and 2) J&J vaccine being approved for widespread administering – on the same page, and not a peep about this in fact being the very same company!
Well, because presumably the companies are staffed sub-c-suite by bona fide scientists doing their best, not gangsters.
Even the ~criminal organisations~ meme is a bit out of touch. Organised criminal enterprises (eg yakuza) for example are not just tolerated but trusted because of what they give back to their local communities, even if they do so purely out of self-interest.
It’s a prejudicial framework of limited epistemic usefulness when it comes to evaluating the merits of these vaccines, imo.
“Vaccine hesitant” checking in. I agree with many of comments proceeding mine regarding lack of trust in what I agree are criminal pharma companies and lack of trust in the CDC. I think the example — but not the only example — of why I am not willing to put my faith in them or any of their vaccines comes from them all suppressing any of the various covid-19 outpatient treatments, most of all ivermectin, as reported by this very site. These are organizations that are not following the science, because if they did, we would have heard about these treatments. They clearly do not care about us. It certainly seems like all they care about is making billions of dollars while people unnecessarily suffer and die due to withholding a vital, inexpensive, life-saving treatment. Remember, if we had been told about these treatments, hundreds of thousands of lives could have been saved!
But there’s more. The more I research around on the internet, the more I see that there are likely dangers to these vaccines beyond just the one we’re told about, which is anaphylaxis. People have suddenly died within 24 hours after receiving these vaccines, including the mRNA vaccines. Some of the people who died were healthy young people in their teens and twenties who almost certainly would have survived covid-19. I don’t know how many there are or how frequently it happens because I don’t think there’s any trustworthy data out there, but if estimates about what percentage of these events actually get reported is true, then it easily could number in the thousands or even tens of thousands. And then there are the people that develop serious debilitating conditions, possibly permanent ones, after receiving the vaccines. They are out there, and along with the deaths they’re not being reported on in the mainstream news. (Which relatedly receives much of its advertising money from these very same criminal big pharama companies! Conflicts of interest abound!) Again, I don’t know how likely it is, and it may just be a scant few hundred cases in the US among the millions that have received the vaccine. But it could be a lot more. What we do know is that there are a lot of incidents reported in the VAERS database now, this database typically only covers a small percentage of the actual adverse events, both doctors and patients have reported on the pushback they receive about casting even the slightest reasonable doubt on the safety of these vaccines, and there is historical precedence for a significantly smaller number of serious adverse events halting a mass vaccination campaign. More reason for me to thoroughly distrust these health officials and companies! All signs point to them not caring about the people they’re ostensibly supposed to protect, and instead care about making billions of dollars for powerful, criminal companies.
I am healthy, in my thirties, and have no other conditions that put me at risk of a serious outcome to covid-19. Here are what I see as my options regarding the vaccine:
1. I could refuse the vaccine and choose to weather the virus, if I even contract it, assuming I haven’t already and had an asymptomatic course. In that situation I could take the outpatient treatment as recommended by so many doctors which will significantly reduce my already very low chance of having a severe outcome, using drugs that have proven themselves very, very safe over the course of many decades.
2. I could take the vaccine, which does not have long term safety data. The short term safety data it has was conducted by the very criminal companies that developed the vaccine, so there is a conflict of interest there. On top of that there is reason to believe that the vaccines are not as safe as we’re being told, as stated above. Worse yet, none of these companies have any liability if their product turns out to be dangerous. If I’m injured from the vaccine and require treatment, my insurance won’t cover it because they are not FDA approved!
So I have chosen not to take the vaccine. In light of the above, that doesn’t seem like an irrational decision, does it?
I’ll end this post by mentioning that I try to maintain as open of a mind as I can regarding all of these topics, and if someone has a counter argument to make then I’ll read it and consider it, so long as it’s made in good faith and is not steeped in vitriol or condescension. That ought to be a low bar to clear, but this is the internet, after all.
One of my biggest reasons for being vaccine hesitant right now is what you mentioned, the enormous push back against raising safety concerns. I would feel less reluctant about getting vaccinated if serious side effects were being given serious attention and information was being made widely available about what to do if those side effects occurred, how long they might last, etc etc. Having recently been in a care taking role for a family member who experienced truly horrible side effects for about 2 weeks following their first shot of moderna and having no idea how to properly do that care taking I feel a lot of anger at these institutions who push vaccination and leave one completely unprepared for what can go wrong.
Thankfully the side effects did prove to be temporary but for most of those 2 weeks it was terrifying thinking they might go on indefinitely. In fact I finally found reassurance reading others’ accounts of similar side effects in VAERS and seeing that my relative wasn’t the *only* person to be going through this. I knew people could experience bad side effects but these in particular I hadn’t heard anything about so I felt at first like what if this is entirely unprecedented and nothing can be done to make it stop? So I say this quite wryly but reading entry after entry in VAERS recounting similar events gave me such relief..
See the problem here? Logic says that if: “They” are lying about something, then why would “They” not lie about Everthing, including the potential outcomes for “healthy people in their thirties”!? Where does one stop? If one gets down to that only person I trusted was my straight-talking Uncle Povl, then my life would probably have been shorter, yet more interesting, and probably on YouTube!
PS –
In Sweden they seeing more and more “healthy people in their thirties” in the ICU. Likely because all of the agit-prop tells them that they are “totally safe” (and corona virus is totally not airborne in Sweden because Anders Tegnell said so himself), so, the “people logic” goes: “us being especially healthy under-30’s can just cram together everywhere”.
Covid-19 has a dose dependency and it is airborne. The higher the virus load, the worse the outcome is likely to be. They already lost too many “healthy, young” nurses on rash assumptions made by 3-rd rate flunkies like Anders Tegnell and now they have to ask for assistance from Denmark.
Yep. Anyway I am very hesitant to argue with any vaccine hesitant: it will never be the case that everybody agree on something. I disagree that because hesitance or anti-vaxxers we cannot reach ‘herd immunity’ or eliminate the virus. We just cannot eliminate the virus even if there was an full and fast vaccination program. Vaccination does not fully prevent spread. Because it is airborne and highly transmissible the probability of eliminating on time all reservoirs seems too low to me.
Hesitant will have to admit that, at their own risk, (even the risk of loosing their jobs because they are hesitant) they can go on without being vaccinated and one day receive a lethal dose of SARS CoV 2. Hesitant will need to admit they might not be welcome in some or in many places depending on how the pandemic evolves, even if it is unfair. Hesitant might finally be negatively selected by the population at large, by virus infection or both. Or may be not.
So far, within my contacts I have only found one person, amongst about a hundred, to declare she is hesitant to vaccination,and I live in a region that was heavily hit by Covid between March and June and during this winter as well. My neighbourhood has been closed for months. She must have been called by the health authorities to get her dose though I don’t know if she has rejected it or not but she would be the only amongst a hundred. This is anecdata but I don’t see any reason to worry about vaccine hesitancy so far. So few they are when it comes the moment that they don’t make a significant dent. And they always have the possibility of thinking twice.
I wonder how much of hesitancy is nothing more than posturing.
I would much rather get a killed virus vaccine and am not at all keen about the mRNA vaccines. I would classify myself as hesitant and would have held out longer, but going into a hospital not vaccinated seemed too risky. Albeit I was and still am using my trusty povidone iodine (both as a nose spray and gargle). So this not posturing. I have repeatedly mentioned that 3 or our 4 aides, all of them certified nursing aides, are not vaccinated and are reluctant due to the bad side effects they’ve seen in people they know. Hourly workers cannot take a day or two off to get through them.
What you do, and this is rational, is to have doubts about a wholly new type of vaccine. I also have doubts about it though in my case I have decided that the risk of Covid 19 overwhelms any rare or not so rare possibility that might arise later. Allergies, whatever comes later, and particularly if schemes of repeated immunization are devised. I feel responsible for my decision and will assume the risks of unexpected outcomes. Those that take the opposite decisions will have to assume their consequences.
I think there are people who have no interested in being vaccinated who just don’t tell anyone. I am not keeping my reluctance secret, but when I mentioned it to an acquaintance she told me that she too had no plans to be vaccinated – and that she wasn’t telling people generally. She just told me because I’d told her.
Also, people may be lying to you about having been vaccinated, Ignacio. That happens. People often try to guess what someone wants to hear and then say it. I don’t do that, haha, but that is what social scientists say is common.
I certainly agree with this. I’ve never heard anyone, including the credentialed folk, make a convincing case that complete elimination of SARS-COV-2 is either possible at this point or necessary. Perhaps at the start of the pandemic it could have been done if western countries responded quickly and decisively like many eastern countries did, but that takes us into the realm of speculation.
Further, I would argue that elimination isn’t necessary, and that the pandemic should be over. We have a vaccine that is supposedly quite effective. As I said I’m not one to take these companies’ at their word for the efficacy of the vaccine, but independent studies seem to confirm that they probably have around a 70-80% efficacy at least, which if true is very good for a vaccine — far better than the flu vaccine! And for those who can’t or won’t take the vaccine, we have an outpatient treatment that is around 85% effective at preventing hospitalization, deaths, and spread! By their powers combined we can turn SARS-COV-2 into a mild flu. Sadly the US and other western countries continue to push vaccines as their only solution, most likely for terribly corrupt reasons.
I doubt that many of the vaccine hesitant reading NC operate based on the simplistic logic of if “They” lie about something, then “They” could lie about anything perhaps everything. An efficacy of 94% edged out by 94.5% efficacy claims sound too good to be true. Moderna’s extra 0.5% looks suspicious. As far as I know the large scale phase III testing of these vaccines has been remarkably shy of large scale follow-up data collection. In spite of what should be substantial harvestable data many unresolved largely minimally studied questions linger about the vaccines — effective against variants? effective how long? how many vaccinated become infected — the claimed 6% or more? side-effects frequency and characteristics? If Big Pharma won’t collect data has the CDC or some other agency stepped in to more thoroughly study the vaccines and progress of the flu? Maybe they have, but if so they haven’t published a large scale follow-up study. If Government can come up with the coin to front the Moderna production line, offer a EUA agreement, liability waiver, and guarantee the purchase of vaccines as long as they prove effective, why can’t Government find money to fund an independent large scale study of the vaccines? I could go on. We are told to evaluate the risks of vaccination and decide for ourselves but how can you evaluate risks based on so little solid information? [Sometimes we have to make a choice with little information for evaluating risks. The lack of information about the vaccines is very fishy.]
Government can, the, on a global scale, tiny Danish government does this as a matter of cause, like they always do with any medical treatment or medication used by the health services. It’s just that in America, government works only for (the) business interests (of senators).
Based on their data, the Danish government are only using the Pfizer and Moderna, mRNA-type vaccines, because they found that the Astra Zeneca has a 1/40000 risk of dangerous blood clots and the assume the Johnson and Johnson is the similar, both are based on adeno-virus.
In Denmark’s case, right now, the Astra Zeneca vaccine is deemed to be riskier than Covid-19, because not everyone in Denmark is getting Covid-19 but everyone will be getting the vaccine.
Based on this informatiob, I would go with the mRNA ones rather than the “dead-virus” type.
I’m vaccine hesitant, too, and will continue to try and hold out for as long as I can.
My biggest fear is employer-mandated vaccination which will surely be around the corner, if not happening already. My NJ employer hasn’t mandated COVID vaccines yet but they dropped the mask requirement for fully vaccinated office employees last Friday. There are now only a small handful of employees, myself included, who are still wearing masks in office. I certainly don’t enjoy feeling “singled out” and getting those pesky double stares, though.
The vaccine companies have no liability… but if a person is forced, does the forcer assume liability?
From what I have seen so far, normally OSHA would cover this, but it seems they’ve found a way around this as well. It seems that everyone, except you as a vaccinated person, is immune to any detrimental effects of the vaccine. That alone gives me enough food for thought.
The New York Times had a recent piece on people who don’t trust that the vaccine is actually free.
I’ve been fully vaccinated and had no issues with surprise billing for the vaccine. Nonetheless, considering how rampant surprise medical billing is here in the United States, I understand why some people might be skeptical.
I’ve come across numerous reports of people injured by the covid-19 vaccine having their claims denied by their insurance companies, and having to resort to crowd funding and donations to deal with their new and often serious health issues. Note though that this is unique to the covid-19 vaccines given that they’re not FDA approved, and doesn’t apply to all vaccines.
Do you have a source for your “numerous reports of people injured” claim?
The elephant in the room, that no one wants to see or say, is that Western governance, the public health system, and democracy failed. The long trunk that is waving back and forth that could slam into you, is the sole reliance on mRNA to code an artificial spike protein to induce human immunity to coronavirus. The first treatment of this kind that has been injected into more than half of the population of the USA with no long-term safety or efficacy data. This is the same hubris that engineered DDT, nuclear isotopes, and Thalidomide.
This is a huge gamble that is ignored. If there are safety issues, if there is a fourth wave coronavirus lockdown next winter, or if hacks disrupt food and energy supplies, the unity of the USA likely will be killed off in 2022.
> The unity of the USA likely will be killed off in 2022
Seems a little soon. But yes, and perhaps this is something both parties want.
> The unity of the USA likely will be killed off in 2022
Seems a little soon. But yes, and perhaps this is something both parties want.
Reminds me of something I saw on the Twitter: “If you have one hundred dollars and I have one hundred dollars and a gun, I have two hundred dollars” (and see Warren Mosler on “how to turn litter into money“). So much for Hillary Clinton‘s “places that are optimistic, diverse, dynamic, moving forward”…
I don’t buy this. It completely ignores the non uniform geospatial distribution of Covid cases. Hospitals were more easily overwhelmed in places where large outbreaks occurred first and this is something that has little to do with numbers of hospital beds per thousand habitants. Fear and alarm where higher in such places and that could be the driver of vaccine hesitancy rather than medical response. You might feel like under siege and this changes minds.
This is too hospital-centric, IMO.
Frankly nothing in this article adds up. Their multinomial analysis is typical rubbish. Either (a) They didn’t know what they were doing (in which case they’re guilty of incompetence in using statistical techniques they have zero understanding of, or (b) They DO know what they are doing (solving an equation with two unknowns by allowing the program to make an arbitrary decision normalising one to get a solution) in which case they’re guilty of serious professional misconduct.
xy=8; solve for x. It really isn’t rocket science. It was recognised back in 1985. If authors continue to propogate studies with discrete outcomes and don’t acknowledge how they attempted to separate mean and variance when they are demonstrably and proved to be perfectly confounded they are fools or liars.
The “defence” that “we can’t do that because by nature we only get one source of data” (equation) just doesn’t cut it. There are always other sources – qualitative, expert-driven etc…… Why should I have to read and deconstruct your laughable article when you just can’t be bothered to do the statistics correctly, as set out in 1985, 36 family-blogging years ago. This stuff is set out in the small print to logit and/or probit sections of the manuals to Stata and other packages. No excuses. Crapification in analysis.
It seems that the spike protein itself may be a toxin, and that there is now evidence that it can get into circulation after vaccination with the mRNA vaccines. Count me amongst the hesitant because, awaiting more data.
Sorry, had trouble linking to the video.
https://m.youtube.com/watch?v=Sis1Sddzbqk