Yves here. The problem with mask use is that in our terribly selfish libertarian-oriented culture, doing something for the benefit of others is a hard sell. Masks reduce contagion but have a meaningful impact only if widely used. Only a lucky few can lay hands on a fitted N95 mask, which would protect the wearer well; N/KN95s that leak, which most do, are presumably better than a procedure-type mask but I am not sure how much.
I have taken to wearing double four ply procedure masks with a badger seal as maybe better than a KN95 that leaks, but I have no way of knowing either way (the badger seal does not exert enough pressure to seal the tougher material in a N/KN95, otherwise I’d go that route).
And I actually have in my possession a super duper mask. But if I tried wearing it on an airplane, some nervous passenger would probably demand I be kicked off as a presumed terrorist.

By Niels-Jakob Hansen, Economist, IMF and Rui C. Mano, Senior Economist, IMF. Originally published at VoxEU
The emergence of new Covid-19 variants and a highly uneven vaccine rollout have put mask mandates back on the policy agenda. This column presents new evidence that state-level mask mandates reduced new weekly COVID-19 cases, hospital admissions, and deaths significantly in the US. The results imply that 87,000 lives were saved up until 19 December 2020, while an additional 58,000 lives could have been saved if all states had put in place a mandate starting in April 2020. Mask mandates had a greater effect in counties more positively inclined towards mask wearing.
The rapid spread of COVID-19 in 2020 prompted a series of unprecedented policy measures. One such measure was mandating the use of face coverings or masks. Many countries and sub-national authorities resorted to the policy. Widespread mask wearing – unlike strict lockdown measures – allows for continued human interaction and economic activity. It is thus of both human and macroeconomic relevance.
With the rollout of vaccines in primarily advanced economies, mask mandates were phased out in many places. However, as the COVID-19 delta variant became prevalent, health authorities are learning that breakthrough infections in vaccinated people are more common than anticipated.1 This coupled with vaccine hesitancy in some parts of the world has put mask mandates again at the centre of the debate.
So Do Mask Mandates Save Lives?
The re-emergence of mask mandates in the policy debate has underscored the need for evidence on their effectiveness. Mask mandates may reduce the transmission of COVID-19 directly by inducing greater mask usage, which lowers the transmission of airborne diseases (Greenhalgh et al, 2020 provides a survey of the evidence). Mask mandates can potentially also work indirectly, by inducing behavioural changes that reduce infection risks (such as physical distancing). However, for the policymaker, the important question is whether mandating mask wearing is effective in curbing the pandemic.
The experience in 2020 provides precious data for identifying the effect of mask mandates. However, using these data to get credible estimates is not trivial. The greatest challenge for identification is that the decision to impose a mask mandate is likely not exogenous and depends on the severity of the pandemic at the local level. Several existing studies have tackled the question using a variety of methods (Chernozhukov et al. 2021, Leech et al. 2021, Lyu and Wehby 2020, Mitze et al. 2020, Renne et al. 2020).
Methodology
In a recent working paper (Hansen and Mano 2021), we contribute to the debate by assessing the effects of US state-level mask mandates using a quasi-experimental setup that allows for a causal interpretation – a regression discontinuity design. Conceptually, we also add to existing studies by finding that mask mandates have markedly different effects depending crucially on the attitudes towards mask wearing. These conditional effects are critical to obtaining credible effects.
Figure 1 illustrates our approach. The map shows counties in and around New Mexico. The colour scheme relates to mask mandates in place on 1 June 2020, as an illustration. Counties with a mask mandate are shown in green; at this time, only New Mexico had a mandate in this region, so all of the ‘greens’ are in New Mexico. Neighbouring counties that do not have a mask mandate and are shown in red. You can think of the border between greens and reds as a ‘mask border’. So, what is the identification idea? We zoom into these ‘mask borders’ and look at COVID-19 outcomes across reds and greens, and we ignore counties in white that are far from the ‘mask border’. Counties around these mask borders are likely to be in the same local stage of the pandemic. The border is random from their perspective, and so is the mask mandate policy.
Figure 1 Counties subject to state-wide mask mandates in and around New Mexico on 1 June 2020
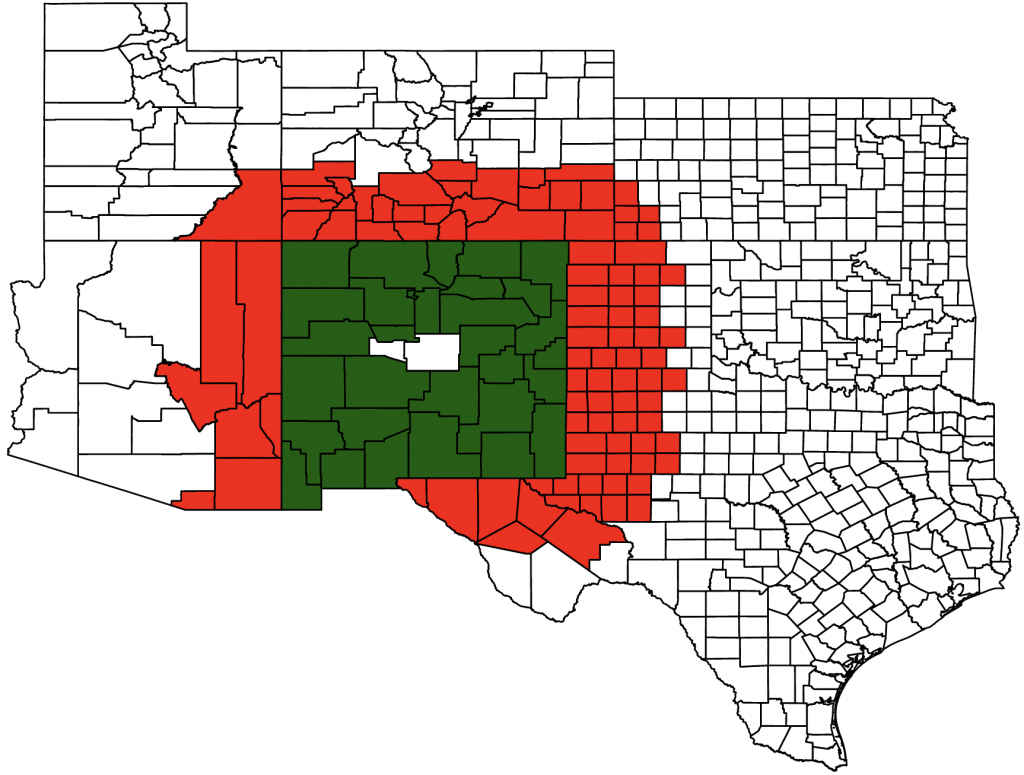
Notes: The map shows counties in New Mexico and the neighbouring states of Arizona, Utah, Colorado, Kansas, Oklahoma and Texas. Counties are coloured (i) white if they are beyond 150 miles from the “mask border”; (ii) red if they are within 150 miles from the ‘mask border’ and do not have a mask mandate; and (iii) green if they are within 150 miles from the ‘mask border’ and have a mask mandate.
Source: Hansen and Mano (2021).
Thinking beyond that particular mask border, Figure 2 shows raw data for COVID-19 outcomes for all weeks in 2020 up to December 19, across all mask borders. The horizontal axis shows a county’s distance to a county without a mask mandate. Imagine driving through the US and starting at the far left on the horizontal axis at -150 miles – the reader would be in a county coloured red in Figure 1. As one drives towards a state that has a mask mandate, the distance to the mask border declines until it reaches zero, meaning a mask border has just been crossed. Now the reader is in a county coloured green in Figure 1. Continuing to drive, one leaves the mask border behind and gets deeper into ‘green’ territory. What happened when the reader crossed the mask border? The vertical axis shows the number of new weekly covid-19 cases per 100,000 inhabitants. There seems to be a discontinuity at the border – the number of new cases per 100,000 inhabitants drops from around 160 to around 110. Similarly, the number of new deaths per 100,000 inhabitants also drops markedly. These are just raw data, without any controls.2
Figure 2 New weekly COVID-19 cases (left) and deaths (right) per 100,000 inhabitants
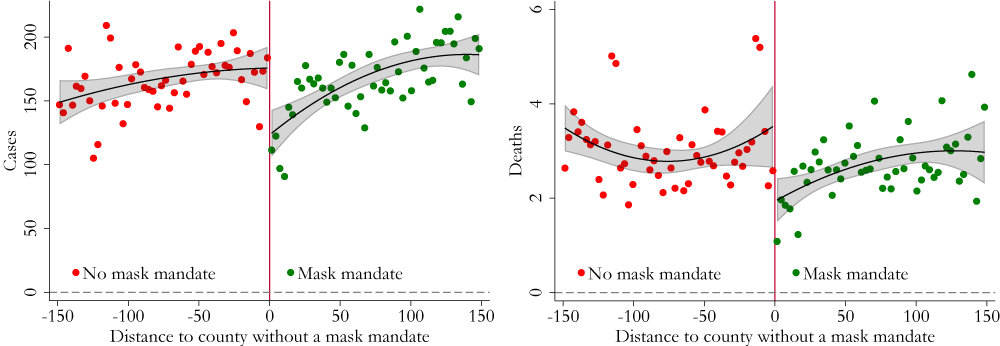
Note: These charts show raw data of new weekly COVID-19 cases and deaths and thus do not account for county or time fixed effects as done in our econometric analysis. Data are binned in intervals of three miles.
Source: Hansen and Mano (2021).
Findings
Going from raw data to an econometric model, we find that mask mandates on average reduced new weekly COVID-19 cases, hospital admissions, and deaths by 55, 11, and 0.7 per 100,000 inhabitants, respectively (Figure 3). To put these numbers in perspective, the average new cases, hospital admissions, and new deaths in our sample are 166, 24, and 2.6. This implies that mask mandates reduced the average weekly COVID-19 cases, hospital admissions, and deaths by roughly a third, a half, and a quarter, respectively. Our results are robust to several robustness checks. Importantly, our results are not driven by other contemporaneous state-level health and containment policies or the existence of county-level mandates in states without state-wide mandates.
Figure 3 Effects of masks mandates on new weekly COVID-19 cases, hospital admissions, and deaths per 100,000 inhabitants
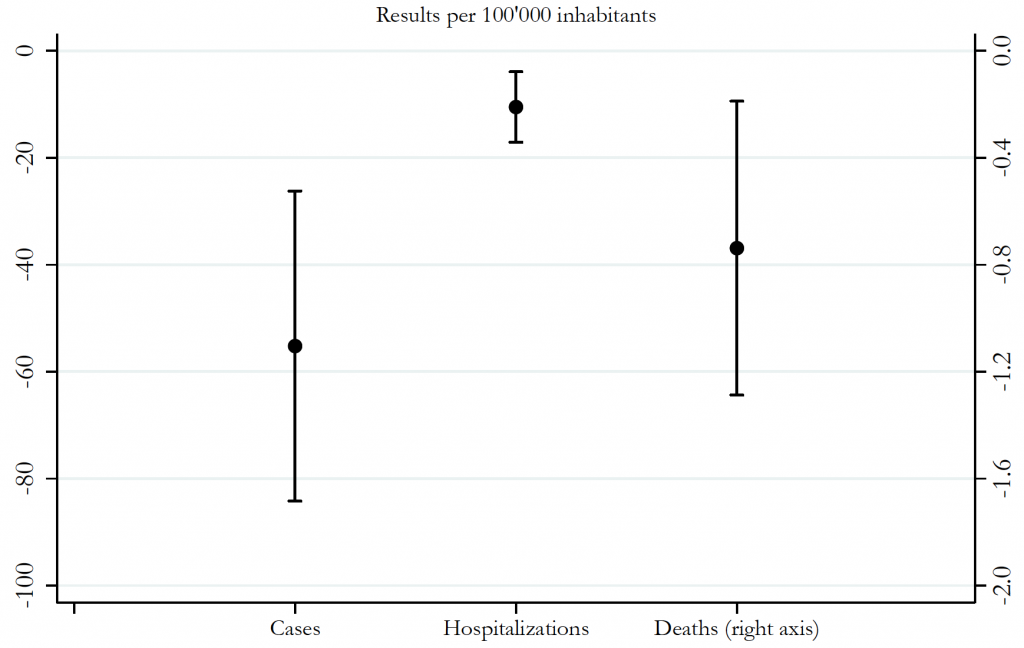
Note: The figure shows the estimated effect (and 90% confidence interval) of state-wide mandates on new weekly COVID-19 cases, hospital admissions, and deaths.
Source: Hansen and Mano (2021).
We also find that estimated effects vary strongly with attitudes towards mask wearing, which themselves vary significantly across the population (Milosh et al., 2020). Such conditional effects are important enough that they must be taken into account. Indeed, the estimated effect of mask mandates on weekly deaths per 100,000 varies from around -2.5 to 0 across our sample of counties, compared to the average effect of -0.7 mentioned above.
Our results imply that mask mandates saved 87,000 lives through 19 December 2020, while an additional 58,000 lives could have been saved in the same period if all states had put in place a mandate starting in April 2020. The magnitude of these effects is large – COVID-19 deaths in the same period amounted to around 309,000 in the US. And yet, these are likely to be lower bound estimates. Indeed, states imposing mask mandates are often reacting to relatively worse outbursts of the pandemic. This would lead us to find smaller differences between counties with and without mandates.
Implications
Since 2020, the deployment of vaccines against COVID-19 is a major advance in the battle against the pandemic. Vaccines are highly effective at reducing serious complications from a COVID-19 infection, and can even reduce transmission. Still, mask mandates remain a highly relevant tool in the years to come. First, not all countries have the same access to vaccines and, even in countries with ample supply, the demand for vaccines is hampered by hesitancy. Second, there is already some evidence that newer variants of the virus can generate breakthrough infections even in vaccinated individuals, meaning vaccine efficacy may decline over time.
Authors’ note: The views expressed in this column are those of the authors and do not necessarily represent the views of the IMF, its Executive Board, or IMF management.
See original post for references


Indeed. Put it in the other way around: if masks weren’t available and mandated in some instances, many, including me, would do less activities due to perceived risk. But even when masks are mandated in some occasions, for instance eating out in restaurants (indoors), masks are less useful. Other circumstances apply: massive events etc.
Uh…what? I lived in Nuevo for many years and I am familiar with it’s ethnic/racial and urban/rural divides. Arguably (and I argue with myself a lot) the most fascinating and interesting place I ever lived. But I am having difficulty wrapping my head around this analysis. Here we have a couple of Euro/IMF analysts of unknown familiarity with the state extrapolating uncorrected macro data from the state and nearby states to postulate national probabilities. When I was studying sadistics in Nuevo I got a “B”. Maybe that accounts for my head scratching.
A question for you: they assume early on that the border is a random event, is that reasonable?
Although the graphs show a visible ‘border effect’ (i.e., different new weekly case rates and death rates), this difference doesn’t hold at distances from the border. IOW, there doesn’t seem to be a differences in the measured outcome (case rates, or death rates) versus mandates or non-mandates.
So I too am scratching my head. Intuitively I believe in masks, but I wouldn’t use this paper to back this belief.
This is an effectiveness of different mask types study I read a few days ago.
https://aip.scitation.org/doi/10.1063/5.0057100
I do worry about spreading stuff to others but I also care about how well different masks work at blocking virus aerosols and also at blocking particles like various industrial dusts. This quote from the study you referenced leaves me cold:
“Furthermore, although the present study does not characterize the effectiveness of masks during inhalation, the aforementioned loss of filtration efficiency due to perimeter leakage is also expected to be present during inhalation, although it is to a lesser extent due to the improved sealing effect produced by the negative pressure difference relation to the ambient.”
I would qualify this study as at best half a study.
I will wear the mask IF I can have the Ivermectin OTC.
CHOOSE.
Both.
And I actually have in my possession a super duper mask. But if I tried wearing it on an airplane, some nervous passenger would probably demand I be kicked off as a presumed terrorist. Yves
That appears to be a respirator with a one-way exhaust port that is normally unfiltered since filtering the exhaust causes back-pressure that tends to defeat the purpose of the exhaust port which is to relieve exhalation pressure under the mask without breaking the mask-to-face seal.
I’ve read* that airlines don’t allow (per the CDC?) such excellent self-protection because those masks make no pretense of protecting others but only the wearer.
*eg. https://www.fox5ny.com/news/why-airlines-banned-masks-with-exhalation-valves
Yes I have said respirator–if that is what is being referred to–and it has a little plastic flap that opens when you exhale–no filtering. But isn’t that also true of the N95? I’ve never owned one.
Of course if you believe droplets are the enemy then the respirator or n95 will stop a sneeze from spraying out of your mouth.
I’ve also tried double masking with paper mask under and cloth mask over but worry that so many layers simply force the air out the sides and perhaps on the inhale as well. Intuitively a paper mask with the Badger seal might be best since no leakage in either direction and more porous.
K or N95s come with or without exhale devices.
OK thanks. Guess I could also put a filter on my respirator port but wearing it would make me look like I was expecting and attack of mustard gas. It makes for a very retro look.
The exhale vent is on N95 masks intended for industrial use. Those were the ONLY high-grade masks I had on hand at the beginning of the epidemic. We used them by blocking the vent with a piece of packing tape, which wasn’t obvious outside the mask. Blocking the vent made the masks much less pleasant to wear.
Medical-grade N95’s (or any medical grade mask) have never had exhale vents. US-designed Medical certified masks are also green colored, most industrial masks are white. If the mask hasn’t been fully tested/certified IN THE US for medical use, the manufacturers keep it white, even if the construction is identical to a medical-spec mask.
If you’re an engineer who’s familiar or trained in the use of respirators you’d have known that blocking the exhaust port is your hasty test for fit, known as a “user seal test” that you’re supposed to do periodically.
You know you got it right when it requires a strong exhalation to cause the mask to lift off and leak (e.g. a positive pressure test). If you can breath with the port covered then the seal to your face is no good.
So walking around with the port covered means for an aerosol you’ve fundamentally defeated the point of an attempt at protecting anyone. Either you’re leaking your cooties or inhaling someone else’s.
I went full prepper late February in 2020 and I regret some things but I did grab a half face respirator seen on contractors all the time with the N95 cartridges. It was one of the last few at Lowes.
You can’t breath out of the cartridges but through the exhaust valve.
So I just cut out two layers of thick cloth and taped em’ over it.
Mission accomplished.
If your half face respirator is airtight against your face then it might be better than wearing a standard cloth mask, since little air leakage goes by your cheeks or nose. Just worry about the exhaust valve.
Just throw a flimsy hospital mask or even bandana over the vent?
Thank you for this. I’m going through a bit of a personal covid crisis at the moment, insofar as it’s weighing heavily on my mind. I’ve been writing compulsively all day. A couple of things re: masks that I’d like to share quickly, all somewhat repetitiously echoing comments I’ve made in the last couple of weeks or so, so apologies for that.
—
First, I asked this in water cooler earlier today (Australia-time) and I’ll put it to the commentariat again to hopefully solicit some thoughtful discussion:
—
Second, a month or so ago when I was arguing with some Sweden stans, I shared this study: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0253510
The key takeaway is this: The lockdown itself didn’t cause the case numbers to decline and allow Melbourne to reach Zero Covid, which we did. Case numbers only declines once the mask mandate was introduced alongside. I agree with this conclusion. Based on my ~lived experience~, the mask mandate worked in Melbourne during our long lockdown last year. This is indisputable in my opinion.
Now, delta has arrived and case numbers are going up. We’re in a lockdown with the same mask mandate. Case numbers are not going down. We’re now being told categorically that masks don’t work with delta.
I can assure you from my observations, the standard of masking in Melbourne is really bad right now. It’s not, in my opinion, because masks are politically cursed here to the same extent that they are in America. We were – rightly – so, so proud of what we were able to do together last year. It’s because public health guidance is lagging behind the medical intelligence we’ve gathered for delta, which I think can be summarised thusly: 1. it’s more transmissible because of the higher viral load of the infected, 2. consequently, there is a greater risk of catching it with rudimentary masking, including outdoors, especially in crowded areas where people are exercising.
I have seen the following, almost every day for the last several weeks:
– poorly fit surgical masks
– well fit and poorly fit cloth masks, of indeterminate material
– people wearing their masks under their nostrils
– people taking their masks away from their mouth when they’re not talking to someone
– countless unmasked exercisers on busy exercise paths
– very (very) few N95 masks amongst the general public
– absolutely no double masking, myself excluded
Suffice it to say that if someone is claiming that ‘masks don’t work’ when that is the case, then there is some chicanery going on.
I asked Yaneer Bar-Yam, of endcoronavirus.org and this banger, the following on the twitter:
His reply was commendably short and to-the-point.
Earlier today I constructed an analogy which I think could be useful in understanding this (I despise bad analogies, especially on the internet, so I’m pretty pleased with this):
(strictly rhetorical point: the analogy is imperfect because, for it to be perfect, there would have to be some point in the past where using your seatbelt in that way *did* confer some protection. nevertheless.)
Consider these rhetorical points. I offer no answers here. Just have a think about the premises. Do you think we would be throwing in the towel so easily if:
a) no viable vaccine existed as was the case in 2020, and we didn’t assume that they offered some kind of long-term sanctuary that we could see on the 70% horizon (set aside any concerns you might have about the safety or the efficacy of the vaccines for the moment)
b) if all other variables were the same, but the virus had a more obviously visceral, deleterious effect on one’s health, such as for example Ebola, pre-treatment AIDS, or some hypothetical virus that wantonly caused gangrene?
c) I think I had another one to put here but my brain has kind of glazed over so I’ll leave it at that.
We need to War Keynes the shit out of N95 masks and mask braces, and distribute them to every resident in this country. You don’t even need to subscribe to MMT to understand that this is plainly, uncontroversially possible: we’re seeing it with vaccine distribution right now. I bet I know which is cheaper.
I’ve ordered the materials per the University Wisconsin-Madison website to make their ‘badger seal’ mask braces at home, which hopefully I have sufficient competence to be able to do. If it turns out I can, then, I’d be more than happy to send them, gratis, to any Australian and Kiwi readers, but I don’t think I’ll have all the materials until later this month. It is of course supremely moronic that we have to grassroots this but such is the neoliberal ghoulscape we have chosen for ourselves.
I don’t like wearing masks. My skin is highly sensitive. I don’t like getting snotty behind the mask and not being able to do anything about it indoors. I miss full-face flirting. I advocate for their proper usage because I believe doing so will mean that we will subsequently be able to go a long time without wearing them. This was exactly Melbourne’s experience from October to June this year.
Cheers and stay safe
Basil Pesto, apologies I don’t have the article at hand, but I believe Lambert posted a while back a discussion about the space between the two masks in a double masking scenario – that just as double framed windows give further insulation against the cold, if a person is breathing into that inner environment, the study measured how warm and humid that will get (I feel it myself when I double mask). So, that would be an environment anti-hospitable to the virus if indeed it was sucked in. Hypothetical, but to me it made sense.
On the math of double masking, the effectiveness is not to be multiplied. They are additive assuming their function is independent, but the second one only applies to the remainder of the first.
If the first mask is 10% effective (M1) , the second mask (M2) will only affect (1-M1)*M2 and the total is M1 + (1-M1)*M2 which is 19%
Thank you! So, if the masks are 90% effective instead of 10% then, using that formula, would that mean that the double masking is 99% effective?
Well, not quite, because the masks are not really independent.
This math is the ideal case. Supposing we were talking about filtering water pouring through one filter after another completely independently. With masks though, they can interfere with each other, so maybe the second mask causes more leakage to the first. With exhaust ports being eliminated, maybe the seal with the extra layer is harder to maintain when breathing out. Or maybe the humidity between the masks actually helps reduce the spread.
On the latter, I believe that the way higher humidity affects virus spread is due to the physiology of breathing and not the virus lifespan in the air. I think humans are more resistant to airborne viruses in higher humidity environments, but that is very anecdotal and I’ve done no research on that.
Sorry not quite that simple. The rule breaks down if the materials are not truly “orthogonal” in stopping particles…. In lay terms, if the particle can get through mask 1 and has some correlation in getting through mask 2 then the maths gets messy.
This is why “totally different fabric types” are preferred in multi layer masks. …. They work totally differently. A polyethylene blend with appropriate spinning of layers (one mask) like dad makes can have very high protective ability. Not to top notch like the suits you see in movies but good enough on day to day usage if you could with sensible mixing. However if Boris doesn’t want to bother testing for mean and variance then we don’t get onto his frequent call list on his phone…..yes we’re bitter.
thanks!
There are unfortunately more complicating factors like touching your mask and eyes. The silver lining to my blepharitis is that years of practice mean I am good at not touching my eyes. Most people don’t realise how often they do it. It’s phenomenally good way to get infection.
yep! don’t worry, I’m definitely aware that I’m massively oversimplifying just for the sake of trying to understand the potential benefit that double masking might confer just based on the basic principles of the technique.
On that though, I remember reading recently that early worries about face-touching while wearing masks doing more harm than good didn’t really bear out, and that face touching tended to be less common in the masked than the unmasked – perhaps it was Tricia Greenhaig’s mask paper?
While the PMC hive mind seems to have determined that mandating injections is good, mandating non-invasive and effective masking is off the table. I don’t like this timeline, and I wish the showrunners would change it.
People in the US object to either mandate at about the same rates, might as well flip a coin and pick one.
I’m being glib but throughout the pandemic the only way people seemed to have learned is through failure. The “all in” vaccine strategy is gonna have to fail before country changes course.
For some reason they may be hesitant to use the very effective “wear a mask to protect yourself from this escaped mutated government bio weapon” line
The problem with mask use is that in our terribly selfish libertarian-oriented culture, doing something for the benefit of others is a hard sell.
True, however, the Concept of Negligence and Assault might apply. If one knows that Masks prevent infecting others, then is a refusal to wear a mask an intent to assault?
I’d note the new Texas Abortion law carries some very interesting provisions which could be used as mask law where anyone aiding a attempted abortion becomes liable for a lawsuit by any person.
… and lawsuits by “any person” will soon clog up the court system. Will Texas taxpayers fund more courts/judges or will cases languish for decades?
no, why do you ask?
It’s an interesting legal question. Criminal transmission of dangerous infectious disease is not without precedent.
Maybe we could apply the new Texas Abortion bill’s approach to prevent people being assaulted by non mask wearers.
I posted this earlier, and cannot find the post.
Oops, it has appeared above now. My error and my apologies.
Does anyone have knowledge of how vaccine passports are actually working in the wild? I heard reports from friends in France that it was largely theater. Most restaurants didn’t ask for them and if they did they just glanced at them so they could well have been fakes.
I just imagine there also being all sorts of technological issues; apps not loading, connectivity, data quality, etc.
commenter ‘David’, whom I believe lives in France, commented the other day making the exact same observation.
I do and I did. It’s essentially episodic. I’ve been in two French cities over the last week, and on occasions I was asked for my pass and on other occasions not. I think that large indoor areas such as large restaurants, theatres, cinemas etc. with clearly defined entrances, do generally ask for them. But it’s much less common in informal settings such as terraces of cafés. Essentially, you display the pass on the screen of your telephone and the other person uses a special app to read it and make sure it’s genuine. I think paper passes are accepted as well, though I’ve never seen one.
But in many ways that’s not the point. Although they grumble, the French have taken the point, and rushed to be vaccinated: as of today almost 80% of the population over 12 have had two doses, which is a pretty amazing turn-around from a few months ago. Sometimes cracking the whip appears to work.
Travelled in Ireland with an EU vaccine passport (including QR code). Every restaurant where we ate inside on the entire 17-day trip asked for the passport and the vast majority scanned the QR code (which I assume provides proof of legitimacy).
IN Singapore, as expected, it is enforced systematically and working flawlessly. Every patron flashes his/her Covid contact tracing Token or mobile phone with Covid contact tracing app open and it connects via Bluetooth instantaneously. The Id of the app/token is linked to the nationwide registry of vaccination. “Flashing the token” has become second nature as you have them at the entry and exit of every shopping mall and at the entrance of every shop inside the shopping mall. On top of that, mobile phone records permanently the COVID Id of mobile phone nearby (in a Bluetooth sense). The recording is local to the phone and is only uploaded to central servers when the person is sick to kick start the forward contact tracing. Retention is 2 weeks. To give you an idea of the size of the net, in a normal day where I take public transportation, I have about 5000-10000 “Bluetooth exchange”.
Yes, it looks a little bit too close to Ira Levin’s ”perfect day “ though…
weak finish…
“there is already some evidence that newer variants of the virus can generate breakthrough infections even in vaccinated individuals, meaning vaccine efficacy may decline over time.”
subtract the italicized words, add an “s” to “decline”
et voilà – a true statement
strengthens the pro-mask argument, imho… one which I support.
some of the problem we have is many states arent actually reporting the data right, some cause there isnt funding, some may be manipulating the data they do report
https://www.npr.org/2021/09/01/1032885251/millions-of-people-are-missing-from-cdc-covid-data-as-states-fail-to-report-case
some of its because they are so distributed on how the data gets collected…or not. and passed to the state seems to be a problem. (and some states dont mandate a health department for counties…at all unless its over 1 million in size)
its very hard to tell where we are if we dont have all the data
https://www.npr.org/2021/09/01/1032885251/millions-of-people-are-missing-from-cdc-covid-data-as-states-fail-to-report-case
“I have in my possession a super duper mask. But if I tried wearing it on an airplane, some nervous passenger would probably demand I be kicked off as a presumed terrorist….”
I have been wearing a valved, FFP3, half mask respirator since March 2020, in Northern Germany where people are probably pickier about what you may and may not wear. Some do not like the valve, but that is easy to address. The half mask was not a problem earlier this month on a couple KLM transatlantic flights, and four 1-5 hour U.S. Midwest train journeys. The worst I got was a little teasing by a Dutch immigration agent, who asked if I was going to Chernobyl.
I can write up and send my experiences if you guys are interested.
Add a voice modulator and everyone will think you’re Bane. Just pipe up a few comments about wiping out the PMC and you’ll be lauded :)
Yves and others in the commentariat, I have to wear full and half mask respirators as part of the PPE I use in my job. There are fit tests for masks that can be performed by occupational health professionals and doctors. Of course, for all of those tests you need to be clean shaven and not have piercings that get in the way. Which may be a problem for some people.
Anyway, these tests involve connecting the exhalation ports on the respirator to a device that measures the pressure as an estimate of seal. It will give you an ultimate “go/no-go” gage of whether that mask, in that size, fits your face and performs as needed. There are alternate methods for testing respirator fit and effectiveness. One of these tests that I have also experienced is you put the mask on, you cover your head and upper body in a hood, and some one releases a chemical that makes you cough/choke into the hood. If you have problems breathing in that environment it means your mask didn’t fit well enough to keep the chemical out. Personally, the fogged glasses test is good enough for me. If while I’m talking and wearing a mask I find my glasses fogging up, then I have a leak in the mask.
I’ve found the under armor sports masks fit my face really well for most day to day use. And when I need to for a site or other purposes where covid (or other contamination) is a concern I wear a respirator with filter cartidges that has been fit to my face and proven to work.
Seems like a market for “attractive” (at least non frightening) fitted masks is there somewhere just waiting to be killed off by somewhere else.
Want a better-than-KN95 mask? The 3M 6300 series respirator sells for $15 at Big River Trading Co and around $26 at big box stores. P100 filters ($10 fer four) make it several times better than an N95. https://www.3m.com/3M/en_US/p/d/v000057396/
Haha, says NOT for consumer use. But it looks like no respirator value, correct? You breathe in and out of the filter?
Per the online specifications, it has an exhalation valve (and so it looks to me).
Must have clicked on another one….thanks!
Could use the stuff procedure mask fabric in respirator value. Or just use it only when shopping and going to the gym here in generally maskless Alabama.
I actually made up a powered filtering attachment, that captures the exhaust and passes it thorough a HEPA (absolute) filter. I am not sure it would draw enough for heavy exercise. I tested it on the 17-hour journey to the U.S. My next three weeks in America, I did not use it – and exposed the naked vent. As far as I could tell, people were happy just to see you wearing any kind of mask, but please correct me if I am mistaken!
The reason some respirators say that is because they can impair breathing and so require a cardiopulmonary test and fit test for use. Although for many people if you fill out a simple form you can get approval for the fit test.
P3 masks are better than P2 masks but are not often mentioned. People may find them a pain to wear. I think they are more or less widely available, at least the last time I looked.
Since masking ought to impact other airborne viral respiratory illnesses, that would be a check on this study. Did they examine influenza over the same period? If this is robust, it should show up in flu data.
Flu data for Australia for 2020-21 is actually pretty amazing.
There is a less well known benefit against respiratory illnesses of wearing a mask. The wearer rebreathes moisture they would have otherwise lost during exhalation. This elevates the humidity in your airways and improves the mucus and respiratory immune responses.
https://www.nih.gov/news-events/news-releases/researchers-propose-humidity-masks-may-lessen-severity-covid-19