By Lambert Strether of Corrente.
Let’s start with the context: Norway returned to “normal daily life,” as their Prime Minister Erna Solberg put it, on September 25, 2021. Normal life didn’t begin well. From the Associated Press, “Rowdy celebrations erupt in Norway as COVID restrictions end”:
Police in Norway on Sunday reported dozens of disturbances and violent clashes including mass brawls in the Nordic country’s big cities after streets, bars, restaurants and nightclubs were filled with people. Long lines were seen outside Oslo’s nightclubs, bars and restaurants late Saturday and police registered at least 50 fights and disturbances during the night.
Neither vaccination status certificates nor negative test results are required to enter such venues in Norway.
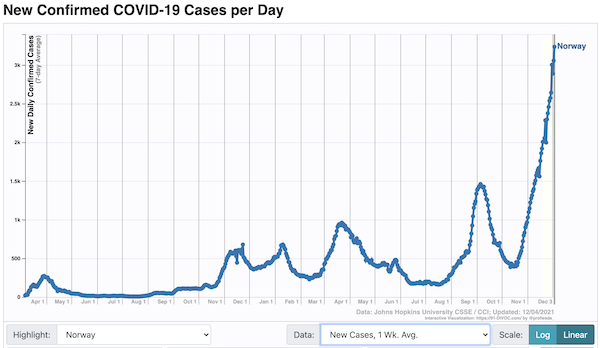
And normal life didn’t continue well. Here is Norway’s case count since that date:
Most of these cases are Delta, but now surely some are Omicron:
Now, normal life has gotten worse. From the Wall Street Journal, “Omicron Cases at Norway Christmas Party Provide Clues on New Variant’s Spread“:
Before Scatec AS A, a Norway-based renewable-energy company, hosted the annual holiday party [on November 26], it took all the major safety precautions, said Stian Tvede Karlsen, a company spokesman. Only vaccinated employees were invited. All had to take a rapid test the day before. The party, at Louise, an upscale Oslo restaurant serving seafood and Scandinavian fare, included about 120 people, several of whom had just returned from South Africa, where the company has a solar-panel project.
More than half of those present have since tested positive for Covid-19, with at least 13 confirmed to have the new variant in what appears to be the world’s biggest Omicron outbreak outside southern Africa—and a glimpse into how it fares in a highly-vaccinated population.
The Oslo municipal health department said it expects more Omicron cases to be confirmed among the 64 Covid-19 cases as medical workers test the remaining patients.
The cluster is remarkable because it took place in a bubble of immunized people, in a country where more than 80% of adults are fully vaccinated.
(As it turns out, 100 of the 120 were infected: 83%.) Louise’s was, of course, a superspreading event. As the Journal says:
An hourslong party with lots of guests talking to each other in a closed, indoor and insulated environment would make for an ideal superspreader event, even for earlier variants of the coronavirus, said Alexandra Phelan, an assistant professor of global and public-health law and ethics at Georgetown University.
And so Norway’s normal has become the abnormal once again:
From Friday morning, mask mandates that had been lifted are back in place, private indoor gatherings are limited to fewer than 100 people, office workers are encouraged to work from home, and bars are operating at reduced capacity.
The capital, Oslo, has canceled a major Christmas gathering and other holiday events are being called off as well.
(Of course, it’s hard to imagine the United States doing any of these things when our time comes.) In this post, I’m going to unpack the notion of superspreading (and superspreaders)[1]. This may help you gracefully bow out from your office Christmas Party, if you have one (I don’t, and I can tell you I don’t miss them a bit). Superspreading also has implications for the Biden Administration’s Vax Only policy, as we shall see.
Here is Nature’s image of a prime venue for a superspreading event:

And here is an image of Louise[2], the Oslo restaurant where the superspreading event took place:

Note the similarities. (The scene from Louise is a dance, not a Christmas Party, but 120 people would still make a crowd.) Perhaps the best way to summarize them is to say that both venues violate the Japanese commonsense guidelines for avoiding Covid: the 3 C’s:
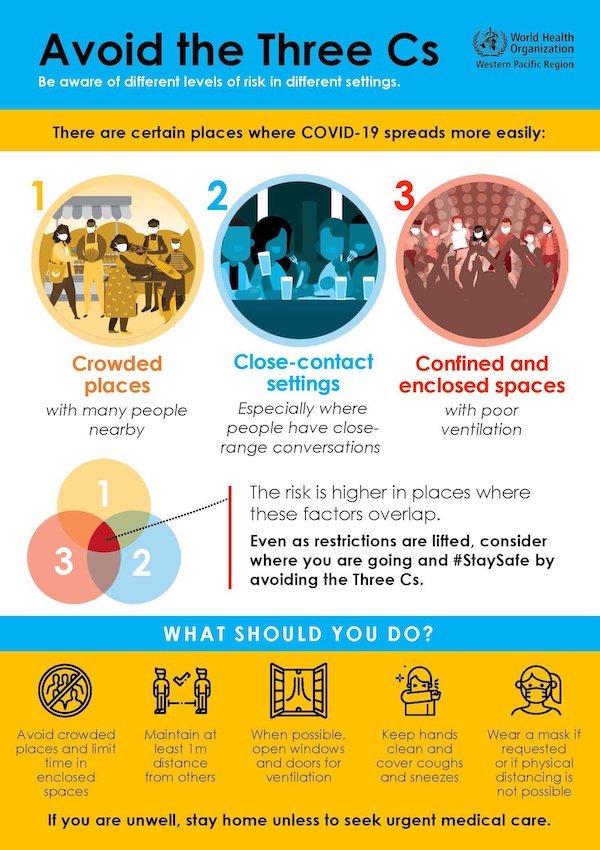
Avoiding Crowded places, Close contact settings, and Confined and enclosed spaces — like company Christmas parties at restaurants or bars — are key tactics to achieve one strategic objective: since Covid is airborne, don’t share air.[3] As public health Ontario writes in “COVID-19 Transmission Through Large Respiratory Droplets and Aerosols… What We Know So Far“:
Indoor settings are a predominant risk factor for transmission. In a systematic review of 5 studies, Bulfone et al. (2020) reported that the odds of indoor transmission were 18.7 times (95% confidence interval [CI]: 6.0–57.9) higher than outdoor settings, and less than 10% of infections occurred outdoors. Very few superspreading events have been described from exclusively outdoor exposures. The explanation for this observation is likely multifactorial which includes important differences in ventilation, UV light, humidity, as well as possible differences in behaviour.
Nature, “Superspreading drives the COVID pandemic — and could help to tame it“:
With a year’s worth of data, researchers have amassed ample evidence of some chief ingredients of superspreading events: prolonged indoor gatherings with poor ventilation. Activities such as singing and aerobic exercise, which produce many of the tiny infectious droplets that can be inhaled by others, are also common components.
From El Pais, in “A room, a bar and a classroom: how the coronavirus is spread through the air” (modeled by atmospheric chemist José Luis Jiménez):
But we now know that shouting and singing in indoor, poorly ventilated spaces over a prolonged period of time also increases the risk of contagion. This is because speaking in a loud voice releases 50 times more virus-laden particles than when we don’t speak at all. These aerosols, if not diffused through ventilation, become increasingly concentrated, which increases the risk of infection. Scientists have shown that these particles – which we also release into the atmosphere when simply breathing and which can escape from improperly worn face masks – can infect people who spend more than a few minutes within a five-meter radius of an infected person, depending on the length of time and the nature of the interaction.
So, absent global eradication and with air travel, Prime Minister Erna Solberg’s “return to normal” — that is, vaccination without layered defenses — was bound to produce a superspreading event at some point, given humanity’s laudable impulse for conviviality[4]. I believe it was Lake Wobegone’s Pastor Ingqvist who asked the question: “If you didn’t want to go to Milwaukee, why did you get on the train?” Why, indeed.
Having, I hope, given you the tools to resist or at least assess entreaties to party on during the holiday season, let’s now turn to the policy implications of the Oslo superspreading Omicron event for the United States.
As readers know, the Biden Administration has been pursuing what might be called a “Vax Only” Covid policy; non-pharmaceutical interventions are consistently ignored or demeaned[5], and even treatment plays a distinctly subsidiary role. Here are some implications of the Oslo Omicron superspreader event for that policy.
First, it is true that the Administration and have long since abandoned the notion that the vaccines are sterilizing, and with it, the notion that “you are protected,” as Biden and Walensky both put it. The CDC’s study of “Bear Week” in Provincetown showed that both vaccinated and unvaccinated carried similar nasal loads of the virus, and hence, presumably, transmitted in equal measure. Nevertheless, even though Fauci and other spokesholes have long since moved the goalposts of preventing transmission off the field entirely, 80% infection in a population (n = 120) that is 100% vaccinated must give pause. As the Wall Street Journal writes, given that some of those infected at Louise carried Omicron:
“The big question that this is starting to add data to, at least anecdotal data, is immune evasion,” said Alexandra Phelan, an assistant professor of global and public-health law and ethics at Georgetown University.
Here is one more anecdote on immune evasion:
6 out of 11 confirmed #Omicron cases in Israel so far are triple vaccinated with Pfizer. https://t.co/0xvb0D83a6
— מאיר רובין Meir Rubin (@Meir_Rubin) December 5, 2021
Translating, our mediocre-by-world-standards 59.1% “fully” (doubly) vaccinated could, for all practical purposes, become 0%, if Omicron ends up dominating Delta. It’s very hard for me to think through the political implications of this, other than a Jackpot-like collapse in public trust not only in the public health institutions, but in existing institutions generally. I’ve never seen charts on public trust with a vertical axis that includes negative numbers; perhaps the pollsters should get ready.
Now, the current line is that Omicron infections are “mild” (examples too numerous too mention). After all, ubiquitous transmission doesn’t matter if nobody gets really sick! Of course, this argument is entirely disingenuous; most Covid infections are “mild” already. The real issue is the absolute number of people who are hospitalized; leaving human suffering and death aside, that’s the number to watch to see if the health care system gets overwhelmed. And since all indications are that Omicron is more transmissible than Delta, and if it is indeed immune evasive, we can expect those absolute numbers to be larger than the last wave.
Of course, so far, we don’t have good data that would prove, as opposed to handwave, that in the aggregate Omicron is mild, certainly not in Oslo. From Reuters:
“None of the patients has severe symptoms; none is hospitalised. However, this is not unexpected given the young age of the participants.”
And CNBC:
“It is still too early to say whether the clinical picture of the disease is different in Omicron infections than in Delta infections,” [Preben Aavitsland, a senior physician at the Norwegian Institute of Public Health,] said.
“None of the patients has severe symptoms; none is hospitalised. However, this is not unexpected given the young age of the participants.”
Further, hospitalization is by definition not mild. But from NBC, “Covid-19 hospitalizations rising in South Africa’s omicron hot spot“:
Covid-19 hospitalizations are rising rapidly in a populous South African province where the new omicron variant of the coronavirus has been detected.
Hospitalizations across the country have increased by 63 percent since the beginning of the month, according to data from the country’s National Institute for Communicable Diseases. In Gauteng, a province that includes the country’s largest city, Johannesburg, hospitalizations are up by nearly 400 percent since the beginning of the month, from 120 for the week ending Nov. 6 to 580 for the week ending Saturday.
The South Africa diseases institute, part of the group of researchers and government institutions that first reported the variant to the World Health Organization, said in a statement that omicron cases were found in Gauteng at “a relatively high frequency.”
Finally, even if we grant that Omicron is “mild” in clinical terms, Vax Only takes no account of Long Covid. Vax Only also assumes that the next variant — being bred, even now, in some immuno-compromised pocket; perhaps a homeless camp in California — will also be mild.
In short, the Biden Administration’s Vax Only policy is, at a minimum, insanely risky. In a sane world, we’d have a layered system of defenses, including non-pharmaceutical interventions like ventilation, to protect us until pharmaceutical interventions or treatments can be found. We have none of that; the Biden administration has, in fact, systematically ignored or demeaned NPIs. We are playing Biden Roulette. We have put all our chips on one number. Unfortunately, Covid (and evolution) are the House. And the wheel keeps spinning.
NOTES
[1] I will refrain from riding my hobbyhorse, air travel. Obviously, if the two Scatec employees had not flown to South Africa and back, they would not have carried Omicron with them to Oslo. Further, if they had been quarantined for two weeks, they would not have spread it. But business travel is important! Indeed, and more than human lives, apparently. It would be nice if we could all be as honest and upfront about these issues as Texas Lieutenant Governor Dan Patrick.
[2] I don’t blame the venue. Official guidance on how to avoid superspreading events has been woefully inadequate, partly because of WHO and CDC’s unwillingness to make anything more than vague verbal gestures toward aerosol transmission.
[3] Masking, ventilation, and keeping interactions short are additional tactics, but they all presuppose entering a non-3C venue in the first place. Ditto bubbles. How much of other people’s are you are breathing is known as the “rebreath fraction.” From the Washington Post:
A critical figure, [Richard Corsi, an indoor air quality expert at Portland State University] says, is the “rebreathe fraction,” which refers to the percentage of the air you breathe in that others in the same indoor space recently breathed out. For instance, he has calculated that when the indoor concentration of carbon dioxide reaches 800 parts per million, then each time you breathe in, one percent of the air you inhale has come from the exhalations of others. During a pandemic, that’s an alarming thought.
[4] That’s how I describe matters on a good day. On a bad day, I say that “extroverts are gonna kill us all.”
[5] The policy seems not merely to be “Vax Only,” but these vaccinations only; there’s no talk, for example, of an Operation Warp Speed-like approach to develop nasal vaccines, which hold out the promise of being sterilizing.


Thanks Lambert (why are you working on a Sunday?). We appreciate your updates. But I couldn’t help but notice. In the first picture above everyone is “large”. One chap had a big coat on so it’s hard to tell, but every one of those people has co-morbidities. I’ve been watching the Beatles doc. from 1970. It needs much more editing (less film) but no one – yes visitors, engineers, the fab four, passers by, men, women, no one is obese. Lots of smoking for sure, but out of perhaps 100 people that pass the camera, no one is even pudgy. Wow, how times have changed.
Huh? I would say that only about 20% are borderline obese. The servers are thin. There’s one guy in front in the first image who has big cheekbones and broad shoulders but I would not hazard that he is fat. You can be wide framed and not fat. The woman with him is not fat.
Moreover, even obese does not necessarily = unhealthy save for joint wear. One of my brothers is morbidly obese. Has been for over 15 years. He does not have hypertension, any problems with his heart rate or EKG, or diabetes. Don’t ask me how. He does have gout but as long as he is careful about how he eats, that does not bother him.
I believe Mantid was referring to the ‘Merican big boys/girl in pix 1 rather than all the slim Norwegians in pix 2.
Agree that obese doesn’t equal unhealthy but suspect health care statistics indicate a close correlation between the two and that your brother may be an outlier/exception.
The two pix offer a quite the contrast between “here and there.”
In one scene early in Get Back Ringo asks, “Do you have a couple of pep pills?” Amphetamine use via “diet pills” was absolutely rampant in the sixties music scene, along with metabolisms being jacked-up on nicotine from the constant smoking of cigarettes. Also remember, George Harrison was all of 26; Paul 27; John and Ringo 29 at the time of the Let It Be sessions. People in those days weren’t living long enough to develop some of the co-morbidities that today are causing deaths from Covid.
None of the Oslo super-spreaders (all of whom supposedly provided proof of vaccination for entry to Louise’s) has been hospitalized thus far — the question is whether they have passed to virus on to others with higher risk factors.
This is the fundamental issue: my vaccine protects only me. It does nothing to prevent me from spreading the virus to you.
Meanwhile In China they would be watching and laughing if they weren’t getting encircled themselves by the suicidal stupidity and incompetence of everyone else…
Yeah, Chinese-Serious for sure.
Whatever Xi’s competence level, pace the Noahpinion piece linked to several weeks ago, the West has handed the CCP to mother of all “othering” devices.
Everyone else in the world has had their political leadership elect to make them actually “unclean” with regards to the virus, a nice turbocharger for feelings of cultural superiority.
I remember as a child being told of all the additional vaccinations etc. I would need to get to visit Asia, not that those talking were intending to, but as a marker of cultural superiority.
Here’s how I declined my office holiday party last week: “I unfortunately will not be able to attend. Have fun! Looks like an interesting place”
I live in a place that’s cold in December. I might have gone if the location had somewhere mentioned: (1) visible CO2 monitors where CO2 would not exceed 1000, (2) excellent filters, (3) outside air pumping, (4) a lot of good fans and ventilation, and (5) maybe a humidifier to keep the relative humidity above 40%.
Re; “The real issue is the absolute number of people who are hospitalized; ….”
When, I am infested with, omicron or one of it’s myriad siblings, I will be avoiding the hospital system, like the plague. I can no longer trust them with my life.
Why? Because our hospitals, now, do not follow (1) traditional, (2) adversarial, (3) constantly contested, (4) but usually, collegial Science,
BUT, they, sadly, follow (are owned by) “The Science” which is a financial subsidiary of “The Money”.
> there’s no talk, for example, of an Operation Warp Speed-like approach to develop nasal vaccines, which hold out the promise of being sterilizing.
Well, to be fair, you can’t really talk about OWS (Operation Warp Speed) without saying something kind of positive about Trump. So that can’t possibly happen.
There is a major new development on the Oslo cluster — apparently 30 people got infected after the 100/120 group left.
From the air that was in the room already…
talk about the West reinventing the wheel….
transmission in entertainment venues has been well-documented since the beginning in countries with robust/detailed contact tracing systems, eg Taiwan, Korea, etc.
Oslo temps are running in the teens in the evening. Not many doors or windows would be open.
So when does this approach measles level of reproduction number?
And Omicron has the “susceptible population” part well in hand, it seems.
Basic Reproduction Number
Went Xmas tree shopping this a.m. in a redder part of the county and was shocked to see
that none of the employees and probably fewer than 20% of the customers were masked.
Not a crowded bar scene, but indoors and with choke points where getting up close and personal
with others was impossible to avoid.
This in a county with a close to 10% positivity rate and a pause on in-hospital elective surgeries.
We are doomed, albeit mildly.
Compare the charts and the text at the top:
Sept 1st 50 cases
Sept 1-26th Rapid rise to 1,400 cases
Sept. 26th Covid restrictions relaxed
Oct 1st- Nov 1st Cases peak on Oct 3rd at 1,500 then descend to 400 on Nov 1st
Nov 1st to now Cases rise to 3,500
The pattern is exactly the same as in 2020. But 2020 was damped, possibly becaus of restrictions.
The superspreader event was 3% of a daily total.
To me it appears there is something about the fall/winter social cycle in Norway which is driving the rise-fall-rise but it was accentuated by the relaxation of restrictions. No indication of age or gender patterns. Drinking in Norway is often accompanied by singing. They conserve energy by making buildings tight and recycle the air.
Saint Fauci used to recommend wearing goggles if memory serves me right. Has there been any more research done on the topic of alternative route of infection for Covid?
As much as I detest Toni the Fauci, the eye protection angle does have some logic behind it, especially for folk that may get splatters or aerosolization into their eyes. Say like dentists or surgeons, or anyone subject to the ubiquitous idiots that get right in your face to communicate. The eye’s mucosa may or may not be susceptible, I don’t know, but what’s more important is the tear film that lubricates and washes the eye quite normally drains into your nasal sinuses. It’s why you can taste eye drops, if you’re interested look up the nasolacrimal duct. Bottom line, anything that gets in your eyes winds up in your nose (sinuses) then your throat.
Well , fully vaccinated folks getting infected is no surprise anymore. But these folks passed the quick antigen test too? I was hoping that the rapid tests would still work re Omi (I read some happy noises from the BioGen people on that) but this looks like,,,,,,,,maybe not.
It was one person who brought it in.
So only one person had to give a false negative quick test.
When a false negative test result occurs, is that random or will a subsequent repeat of the same test on the same person be more likely to produce another false negative?
Wondering if one could beat down the false-negative frequency by taking the test multiple times. Of course, I suppose that would increase the likelihood of a false positive in one of the tests.
1) I was wondering if the servers and other support staff had been tested, even if they left before the people came, the virus can survive in the air.
2) The rapid tests aren’t that accurate.
I was also optimistic about rapid tests since they were reported to detect omicron. I wonder if perhaps this variant transmits with a lower viral load than needed to trigger a positive on the rapid tests – ie, do they need to be recalibrated? Hopefully we will learn more quickly.
Note they tested the day before–not immediately prior.
Hi Lambert,
Have you come across Geert Vanden Bosscha’s argument? There are actually two strands. First the idea that vaccinating in a pandemic is likely to select for virus mutations that can evade the vaccine.
The second is that our innate immunity can in most cases handle infection. Sometimes, if the viral load is high, then one may become ill, leading to development of acquired immunity. The innate immunity is strong in the young, but can weaken with age, poor health, diet, disease, etc. So these are factors that will predispose to hospitalisation and mortality.
The issue with mass vaccination is that the innate immunity is suppressed by the vaccinal antibodies. When a new virus mutation comes along, the vaccinal antibodies that are produced, may bind but not neutralise. And in binding, they subdue the innate immunity from acting.
So vaccination means that the vaccinated have a suppressed innate immune system that can no longer act effectively against SARS-COV2. Consequently herd immunity (to protect the vulnerable) can not be achieved, and we are condemned to continual cycles of virus mutation and infection.
There is a pretty clear talk here:
https://www.voiceforscienceandsolidarity.org/videos-and-interviews/the-implication-of-massive-vaccination-during-the-pandemic
The website also has a comprehensive FAQ that lays out the science.
We have not yet seen the variants that will arise from the selective pressure of vaccines.
This one probably began cooking before there were vaccines.
It is, however, being selected for by a lot of convalescent immunity in South Africa, so we should expect to see things like it being selected for by vaccines too. But variants take a long time to generate and manifest themselves, so it’s still too early to make grand conclusions about the vaccines
COVID is a two-phase disease. Or maybe three-phase, see below.
The first phase is the acute infection in the URT — most people manage to handle the infection at that stage by a combination of innate and adaptive immunity. And yes, young people have better innate immunity and also stronger adaptive immune systems too.
Second phase is when it gets in the lower lungs — if you get to that point, you will have problems, even from the cell damage alone. In most people it does not.
But then the real problems are immunopatholigcal in nature — the immune systems goes crazy as a result of the massive cell damage and certain properties of the virus, and then it does most of the rest of the damage.
And old people are much more predisposed to that hyperinflammatory reaction. So are obese people, even when they are not old, which is why they are the other major risk group.
That is absolutely false, where do such nonsensical ideas come from?
He is not arguing that the COVID variants emerged because of vaccines. Rather the mutations were there, but the vaccines naturally selected for delta as it (at least partially) evaded vaccine antibodies.
On ‘suppressed innate immune system” – apologies that was my shorthand. He is saying that S-specific antibodies will out-compete innate antibodies for binding to the spike protein of the virus. With virus variants, these S-specific antibodies may stilll outcompete innate antibodies to bind, but not are not capable of neutralising.
Very interesting. I’d seen him interviewed before, but with less time to make his argument. Although I’m relatively old and had a moderately hard time of it, I’m relieved that I contracted the virus early on, before anyone was masking. No proof, so no movie theaters for me. Like the other scientists and doctors who make the sense, I see Vanden Bosscha is confined to obscure media platforms.
Between that hypothesis and mutations that are, in general outpacing the creation, manufacturing, and distribution of non-sterilizing vaccines, the US is in more trouble.
While two different things, the policy groupthink is related and among peers: think about the war policy (More war = more peace) or the doubling down of stupidity that’s been demonstrated over and over with this invasion and that invasion.
Think of how much evidence against the policies & strategies and the deaths that has accumulated and yet it continues.
Does the fact that Comirnaty has received full FDA approval mean that EUAs cannot be issued for any further newly developed and not yet fully tested therapies?
I wonder if the Four Thieves Vinegar people can develop a safe synthesis route for ‘the antihelminthic drug that must not be named”.
(also of interest, a safe low-tech synthetic route for syrosingopine would be world-changing. I wonder if it can be done)
This just keeps getting more depressing. I would love to have my life back. I miss my neighbors and the people in various businesses that I visited pre covid. I haven’t bothered to decorate for Christmas, no Halloween no chatting with people out and about……there just isn’t anything one can do but sit in the house.
So let’s go Brandon. Biden’s testing program complete joke.
My “small liberal arts college” has put the kibosh on holiday parties, and typical of their communication style sent an email out late friday afternoon regarding the upcoming winter term using “we plan to, but…” to
I don’t envy anyone in the administratium over the next few weeks. The writing is on the wall.
Well I have 3 vaccine shots now. One thing my career educated me on was the danger of inhaling small particles deep into the lungs,whether it be silicates,coal,viruses, or pollution. Went to plenty of safety meeting on the danger of these small particulates. A vaccine and mask wearing was no issue for me. I don’t take risk with these type of things.
Career=Mining
I would expect “leaders” like Biden to double down on vaccinations as that is all they want to do. When a population has reached about 80%, governments can then step back and say that they have done their job. Anything that happens after that time is all on you. Any failures can be pinned on people who are hesitant to be vaccinated and it is also cathartic to punish such people like we are seeing in countries like those in Europe.
Having vaccinations as your strategy means that it is easy for PMC types to see data on their dashboards as in those that have had their first dose, those that are double-dosed and now a new category of those that have had their first booster. You can put these numbers into an Excel program and play around with them by State, by region or whatever way you want to do it to make it look like you are showing progress. But masks, ventilation and social distancing? How do you show them on an Excel sheet? So they will be ignored and it will be all about the vaccines.
Did notice something the past few days and that is the constant mention of the people that have been double-vaccinated but who Omicron still got. I want to keep an eye on this to see if this will become the excuse by our leaders why vaccinations failed. So they would say they were on track to get rid of the pandemic and the Delta strain but unfortunately Omicron came along and blew that strategy out of the water. Who could have seen that development? Yeah, this excuse is pretty weak tea but they will need some sort of excuse for the failure of the vaccine strategy.
All vaccinated,all passed rapid tests,83% positive.
And more variants on the way.
Time to choose a fall Guy/Girl here in the USA, go long reefer trucks and wave ByeBye to what’s left of the healthcare system.
Let’s shine some light on Gautang.
It has several disparate parts, Johannesburg Downtown, the Northern, Southern , Eastern and Western suburbs, and Soweto.
Few live live down town. The suburbs are a combination of apartments and single family residences. Soweto was and probably is “non white”.
Travel to and from Soweto to Johannesburg’s business district was, and probably is, by very crowded trains., or very crowded cars and vans.
In addition there were and probably still are, remnants of crowded non-white townships.
While it is summer in ZA, the process of living in Soweto is to live, travel and work in close contact, busy city.
Because I believe in Lambert’s research on transmission of covid, I cannot be surprised that a crowded African City, with good air connections to the rest of the world has become a breeding ground and epicenter for a Covid.
This is one reason why HIV hit South Africa so hard. It was one of the few Sub-Saharan African countries with good transport links.
I’m sorry but every time I see the good Dr. F on screen proclaiming some sort of edict to remain calm (and go shopping), all I can imagine is this venerable commercial.
I will repent for my insolence later. If I’m around. If there’s anyone left to absolve me.
https://www.youtube.com/watch?v=7Fx9xabEoJo
An Englishman & an Irishman walked into a bar just over a week ago, both wearing masks with the former after a long drive being desperate for a leak. That bar in a small town in Northern Ireland was packed solid with I guess around 300 people, none of whom were masked. Social distancing was of the intimate kind & the place was basically a large sealed box containing a mix of very loud vocals.
The toilet according to Murphy’s law was of course right at the back so there were 2 choices of which pissing oneself in public appeared to be the worst. I met the other fella outside a couple of minutes later & a few days afterwards me & her both went down with something that felt like flu, which of course was very likely pure coincidence & we are fine now.
One bar in one packed town of many bars with Christmas on it’s way will it appears be very welcoming to O if it happens to be walked through the door.
As to vaccine & booster protection 2 Israeli doctors infected – sorry if already featured.
https://www.reuters.com/business/healthcare-pharmaceuticals/two-israeli-doctors-infected-with-omicron-hospital-says-2021-11-30/
I’m sorry to hear its like that in NI, but I think the malign influence from above in the UK makes a difference. From what I can see from talking to my English friends, compliance is far higher in the Republic. I’ve certainly seen a few pubs with widespread movement and non-mask wearing, but in the pubs/restaurants I’ve seen recently most people are masked when moving around and are staying seated, and many pubs still at least try to keep some air circulating. Not ideal, but not terrible either I think.
I think its going to be a disaster here financially for Irish pubs/restaurants. There will be very few formal office events and not many informal ones either. They are hoping I think for a formal shut down so at least they can claim some compensation.
Yesterday a friend in her mid 20’s told me that lots of her friends are cancelling pub outings but are organising small house parties. I guess they want to have fun, they just don’t want to be seen to be too irresponsible. Not that the virus will care.
County Tyrone has been at the epicentre of the pandemic & the fella we went to pick up at the bar only recently got out of hospital after 6 days on oxygen The old fella with me who has to be careful was also shocked but neither of us usually go to bars he being something of a hermit up in Donegal. It felt like a time warp from 2017 being when I last walked through those doors – don’t know if that is the case everywhere else over here but given the relaxing of measures around hospititality it would now not surprise me if it was.
Sacramento calling (apologies to the BBC). My adventure in vaccine-land started last year with the University of Calif, Davis Medical Center which is the big dog in things medical here. Because of age (69) and some genetic issues, I was head of the line and got Pfizer in March of this year with the second dose a few weeks later also at UCD Med. A very professional operation with both doctors and nurses keeping an eye on us and much typing into computers. They checked us carefully both before and after our shots, and we were kept distanced from them and each other.
Oops now we need a booster due to waning efficiency so I tried to return to UCD Med. I was told that they had used up their few booster shots and the doses had all been sent to CVS and WalMart. Not kidding.
So off I went to a Walmart to find an area in front of the pharmacy had some folding chairs set up and a velvet rope on posts setting it aside from pretty much nothing at all. We sat there both before and after getting a booster with no one checking on us. They had some Moderna and no Pfizer. Three staff were there, two of whom were a disaster and one was competent. The little area that the boosters were given in do not accommodate a wheelchair so I just told them to shoot me there with the others sitting around.
The fine print: Please remember that when I was at UCD Med Center there was much typing into computers and double checking the dose and batch numbers of vials and so forth. Walmart tried to find me in a variety (as in plural) of data bases as having had the first two shots and failed. I am not in any data base they were able to access to confirm that I had already had the two doses of vaccine. Walmart was out of Pfizer which is the vaccine I had so I asked for Moderna. I now have two CDC cards, one from UCD showing Pfizer and one from Walmart showing a Moderna booster.
You tell me why all the doses went to CVS and Walmart. You also tell me why I am not in any of the data bases showing my vaccine status. For all anyone knows, all I have is a piece (actually now two pieces) of cardboard. I have no idea why TSA or my local restaurant would believe a piece of cardboard.
Never mind that all this theater and getting shots means nothing much now that we have the new improved Covid, Omicron. The shots and booster made me pretty sick. I recovered but I’m truly concerned about new boosters and risks from them while Omicron is on the march. My current choice is N95 masks made here by Honeywell or 3M and surgical paper tape around the edge so its glued down to my skin (no gaps) plus goggles if I need to communicate. If I don’t need to communicate I use a full face N99 equivalent respirator also made here by 3M. I use disposable gloves and have “outside” shoes that don’t come inside the house when I come back home. And I use the protocols on the FLCCC web site to help prevent viral replication.
It would appear though that Omicron is so wildly infectious that I don’t have a high level of confidence that even those measures and staying home as much as possible will be enough to avoid infection. Two years of this, and we are back to zero. Lordy.
Ana in Sacramento
take a pic on your phone of your cardboard so you won’t lose the “cards.”
Thanks, that is a good idea. After being mad about the whole thing, I gave in. Made some copies to have in the file and got one of those lanyard things with the plastic gizmo and put them both in the gizmo. When I need it out and about, I wear it under my shirt and pull it out to do show and tell with whomever the martinet of the day is.
Ana in Sacto
There is also a website for CA residents to upload your vaccine info to and get a QR code to flash around.
I did the upload but have never used it in public. Health care people should be able to access.
The link didn’t print…
https://myvaccinerecord.cdph.ca.gov/
Thank you, I’m navigating around on the site now. One thing I noted is that they are careful to give out an 800 number and then immediately below the number they state that they cannot update your vaccine record if you call them.
Just too funny. I ran a statewide ombudsman program for a state dept for many years and our 800 number rang on my desk. Those lines are not cheap, and we always always always answered it by the second ring.
Sooo, my tax dollars are paying for an 800 line the California Digital Vaccine Records folks will not use to talk to me to update my vaccine record. Honestly you can’t make this stuff up.
Ana in Sacto
Comment from North Carolina – Our State level “upload site” doesn’t currently have a 3rd slot for the booster info. Our boost (late October) came from Publix Pharmacy. Pharmacist was only able to place a comment in the record… so the printable form (w/ QR code) remains the same as it was..only shows receipt of primary vax 1 & 2…. Worth noting – Made the request to put the boost data in our file last week. Pharmacist said I was the first request he received to actually do a data upload to the “official NC” site…
https://www.usnews.com/news/us/articles/2021-12-05/fauci-says-early-reports-encouraging-about-omicron-variant
“U.S. health officials said Sunday that while the omicron variant of the coronavirus is rapidly spreading throughout the country, early indications suggest it may be less dangerous than delta, which continues to drive a surge of hospitalizations.”
““Thus far, it does not look like there’s a great degree of severity to it,” Fauci said. “But we have really got to be careful before we make any determinations that it is less severe or it really doesn’t cause any severe illness, comparable to delta.””
“Fauci said the Biden administration is considering lifting travel restrictions against noncitizens entering the United States from several African countries. They were imposed as the omicron variant exploded in the region, but U.N. Secretary-General Antonio Guterres has blasted such measures as “travel apartheid.”
No problem guys. Who are we to question Fauci right? I don’t want to be accused of doubting SCIENCE itself.
Thanks.
After almost two years, this is clearly a turning point in the coronavirus pandemic. Relying solely on for-profit mRNA “vaccines” is a failure. They do not prevent transmission. “Superspreading Events” occur among the fully vaccinated in indoor crowds. “30 people got infected after the 100/120 group left”.
Like Stalingrad or Gettysburg defeats, failures to prevent profiteering, no crash programs for alternative treatments, incompetence, and no layered defenses, means the future of the Biden Administration and the fate of the Western Empire rests solely on the Omicron variant. If the virus collapses the privatized healthcare system across the West with overflowing sick patients this winter, the corporate/state Empire falls. Instead, if it is just another cold, the flailing Empire survives to face its next defeat; a war with Russia in Ukraine.
If the coronavirus pandemic ends now with a cold, it will become a forgotten memory of the survivors like the Lost Generation after WWI and the Spanish flu. If not and Omicron destroys the Global Imperialists all by itself, any historians left may remark on the parallels between Western Neoliberals and Ottoman Eunuchs.
Given my witzelsucht (wife’s diagnosis), visualizing the anatomical similarities between neoliberalism’s agents and eunuchs is hilarious, to me at least.
Problem is, even if Omicron is less virulent, it appears to be far more infections than even Delta! So there are plenty of hospitalizations in S Africa, this is not the common cold. Let’s say we are lucky and we have have 25% less hospitalization. 2 to 4x more cases than Delta (including vaccinated population), your looking at a lot more hospitalization than the last wave. Maybe not as many *per capita* as our first wave, but way more cases!
I suspect that there are plenty of people who are pretty sick in addition to those who test positive. I have gone through nine rounds of COVID-19, five rounds before being fully vaccinated and four rounds after being fully vaccinated. I have never been able to pull a positive nasal swab despite being tested every two weeks. Even at times when I had a sore throat and felt sure that I could pull a positive PCR test my tests were negative. I can only guess that I might have been able to pull a positive test during lockdown week, the third week of March 2020, which was the initial infection. For me COVID-19 is utterly debilitating. The fatigue, brain fog, and GI tract problems render me worthless.
One thing that is starting to worry me is that, when I go into the kind of small shop of which there are many here, the shopkeeper will put their mask on before coming to greet me. This is pointless and even counter-productive, but it reflects the fact that most people are still prisoners of the droplet model of contamination, and assume that they can only contaminate others if they are standing close by. I’ve even seen waiters and bar staff unmask when they aren’t with customers. Hard as it may be, I don’t see any alternative to telling people that if they work in confined spaces and mix with others, they have to wear masks all the time. In the end, it’s hard to see the difference between twenty people becoming contaminated all at once, and twenty people becoming contaminated after passing through the same confined space over a period of hours.
Hard as it may be, I don’t see any alternative to telling people that if they work in confined spaces and mix with others, they have to wear masks all the time. David
I’d bet that’s futile given Omicron and the less than 100% effectiveness of masks -UNLESS combined with good ventilation with fresh and/or highly filtered and/or sterilized air. And then, even the intermittent wearing you described might be adequate.
Unless Omicron turns out to be mild, my bet is that it will force fundamental change – not something on-the-cheap at the expense of increasing the discomfort of workers.
This is why I think the refusal of public health authorities to admit they got it so wrong on aersols is so dangerous. Instead, they are stealthily changing advice to make it look like they are listening and on top of of the current science.
The reality is that once a message is out and becomes embedded, as the ‘socially distance and keep your hands clean’ one did, its very hard to change. Public authorities need to communicate that the old message is dead and there is a new one that people must follow. This needs to be hammered into peoples consciousness over and over. But nobody is doing it, largely, I think, because public health authorities don’t want to be seen to admit in public to have gotten the science so badly wrong.
Yes, I see this frequently at cafes, the staff at my apartment etc. Sometimes I try and spread the good word (in as patient and friendly a way I can muster) but it can be a bit ‘in one ear and out the other’. They’ll nod and express gratitude and then, when you see them again, it’s unbraced surgical masks all-round. In that sense I think PK is right (and I agree with all his other observations), these things really do need to be hammered into peoples’ consciousness over and over. I don’t know how else you’re supposed to get these messages across? It can be interesting to see what exactly it takes for people to take information on board. What is it exactly that pushes people over the edge into message acceptance? Is it just lots of people all pulling in one direction, an acceptable consensus? Do TV ads make the difference? It’s really quite mysterious. Many of these people, of course, gleefully made fun of how stupid and malinformed Trump supporters are (to take one example). I know I shouldn’t be surprised by any of this – that people believe they can shape their own reality and the world itself will comply – but I find it deeply troubling almost to the extent that it’s all a bit absurd and funny now.
While infected, 20 months back. We’d worn KF-94 & gloves to fetch groceries, in the lobby. We knew the delivery folks, & were actually discussing PASC symptoms, as a neighbor kinda jumped into the tiny elevator; spewing vituperation at “alarmist,” “conspiracy theories” we were feeding the “essentials!” Of, course she was maskless. “Pandemic,” was apparently a term discouraged by MSNBCNN? So, we were BAD, harshing our better’s beatific delusional grandiosity was anathema; roughly from Li Wenliang’s death, on? We’d followed Italian & East Asian clinicians’ tweets & epidemiologists’ prepub articles, then (so were Rooskibots?)
Sounds to me like customer-driven masking. Enough customers want to see them masked, so they mask in their immediate presence. They are mostly not thinking about modes of transmission. Plenty of such workers would be happy to be unmasked at all times.
Yep, if there is a future it may well turn out that mask mandates (properly fitted N-95 or better which should be mailed to every address) and beefing up ventilation and filtration would have been more effective than vaccine mandates. I share that nougat of wisdom frequently, telling folk TPTB have it backwards, and people think I’m nuts. But then how many mask manufacturers have minted a few instant billionaires? Don’t forget to sing ‘Happy Birthday’ while washing those hands children.
Let’s go Brandon has been very effective convincing folks the vaccines make the masks unnecessary. Flying back to USA from Mexico, I had to present my vaccine card and a recent negative Covid-19 test. No one examined my mask. On the plane many folks bought a drink which they could hold unmasked and sip when a flight attendant came by. The blue poorly fitting masks worn by most with visible gaps rivaled handkerchiefs.
I expected this, and took iVermectina as a prophylactic like the India health care workers. I took two doses 72 hours apart before my flight as described in the India Study. As Dr. John Campbell said, our leaders are not horses or cattle.
Coming late to this conversation, but I have a serious question: what’s the end goal here? We have vaccines. The vaccines don’t stop people from getting infected and spreading the disease, but they have been shown to be very effective at ending hospitalizations and worse. Not perfect mind you, but I have no evidence that anything can be.
So, when do we go back to normal? By that I mean, what are the numbers that say “hey, we can go back to normal now”? What would that entail happening? I could see a combination of vaccinating the entire world and then going into, say, a two-month world-wide lockdown with dramatic levels of testing to ensure the virus is gone altogether. But I tend to think the likelihood of that is zero.
So, assuming it is, then COVID will always be with us. And, if that’s the case, what exactly are we waiting for and how likely is it we’ll see whatever it is we are waiting for in the near (or distant) future?
That’s interesting, because it’s exactly the question I have been waiting for somebody much wiser than me to ask and, with luck, answer. And nothing.
If the “end-state,” as strategists call it, is the eradication of the virus throughout the world, then we might as well give up now. If the transmissibility of the Omicron variant is as bad as they say, and if other variants are going to be as bad if not worse, and if there is no prospect of a sterilising virus, then seven billion people would need to be vaccinated (how many times per year?). This is not going to happen, no matter how many doses of the virus you manufacture and give away. Good luck in trying to vaccinate people to a regular schedule in rural Katanga, in Myanmar, in the slums of Mumbai. And the problem is that with such a contagious virus, it’s enough that a taxi driver in Lubumbashi catches it from his brother, gives it to someone taking a flight to Kinshasa, who gives it to someone taking a flight to Paris who … well, the rest we know already. If by “living with” the virus we mean accepting a situation where sudden outbreaks of new variants arise routinely and kill hundreds of thousands of people, then, well, we need a new definition of “living,” to include dying.
And the answer is what, exactly? The only thing I can imagine is a world-wide ban on travel within and between all states in the world for the indefinite future. Any takers?
So, I’ve been thinking about this since I saw a newscast, where a doctor was interviewed and said our grandchildren and great grandchildren will be dealing with the Coronavirus. Because its not “just going to go away” as our last President so eloquently said.
Vaccines reduce the death rate significantly. Everything I’ve read and heard point in that direction. If that is true then wouldn’t a reasonable end goal be to simply put the elderly and folks with high risk on a continuous cycle of vaccines? And, of course, anyone else who has that desire (I do and would). And have a our national health system maintain a strong focus on quickly identifying new variants and quickly developing new vaccines?
Obviously some significant fraction of the population doesn’t trust the government, science, Fauci, whatever enough to get vaccinated, so they are putting themselves in a position of higher risk (and the rest of us to a much smaller degree). But I can’t see how that changes.
So maybe we are already at the absolute best point we practically can be.
Well, for most folk, especially first world westerners, ‘…accepting a situation where sudden outbreaks…kill hundreds of thousands…’ is pretty abstract. Actually we’re closing in on a million here in ‘murica. As more and more people either succumb themselves or watch their loved ones suffer, surely people will get serious. Who really needs to travel with today’s electronic communication? Apparently Schmuckerberg is gonna soon be able to make us think we’re there, even if we’re not. Most business travel (did you fly in first or business?) is BS, more about getting away from the spouse for a few days and partying hardy (but, but think of the strippers, how will they make a living without all those out of town businessfolk?). Tourism was destructive BS even before the electronic revolution. Of course ya need people to shepherd the container ships across those watery stretches, but they often don’t even get off the boat. So who needs to travel, I mean really needs to? There could be an IgA stimulating intranasal vaccine in development that might be near sterilizing? But let’s say you’re a Pfizer exec (former shareholder here), does a one and your done vaccine that may give protection for a decade or more make business sense. Hell no. Better to rake in all that precious lucre from semiannual boosters. Sky’s the limit?
“As more and more people either succumb themselves or watch their loved ones suffer, surely people will get serious.”
I don’t know. It seems like the people who are anti vaccination are also fatalistic. Negative outcomes are due to “god’s will” or bad luck, and not something that requires a change in behavior.
And I know a lot of people who have been infected and didn’t suffer more than expected. If that is the experience of most people, I think most people won’t care that much. They’ll be happy to let their politics trump their worst potential risk assessments.
I think the short answer is effective treatments like HIV meds
I see virtually no coverage on research on that front
IIRC, it took about 25 years to get effective HIV meds.
I’m just waiting to see if Omicron and Delta spread independently from each other. Meaning if you get one, it doesn’t exclude you from getting the other.
Looks like Michigan and Minnesota will be good proving grounds here. A lot of eastern and central Europe are good candidates, after the recent delta spikes. UK didn’t spike but never went down on weekly cases.
Denmark is kicking Norways butt!
The case fatality rate is staying low, for now. I think that CFR in Sweden is rising, and I assume that they got “the numbers” under control by the infamous FHM instructing that vaccinated shall not be tested for Covid-19 when they show up in the hospitals.
Consequently, I am not going back to the office, and I am not going to the Christmas party either.
Ever again?
In Sweden, yes. I won’t mind going occasionally but I think the demand for “full time office occupancy” is just some KPI-metric management have been saddled with. They seem to be quite driven on this. They are still circling around the core issue, but, I think we will soon be discussing what the off-boarding package should look like.