This is Naked Capitalism fundraising week. 659 donors have already invested in our efforts to combat corruption and predatory conduct, particularly in the financial realm. Please join us and participate via our donation page, which shows how to give via check, credit card, debit card, or PayPal. Read about why we’re doing this fundraiser, what we’ve accomplished in the last year,, and our current goal, rewarding our guest bloggers.
By Lambert Strether of Corrente.
What is infection control? According to the CDC:
Infection control prevents or stops the spread of infections in healthcare settings.
Which, arguably, hospitals are. In fact, hospitals have administrative structures for Hospital Infection Control (HIC). Again the CDC:
The role of the hospital infection control committee (HICC) is to implement the annual infection control programme and policies….
- Develop a system for identifying, reporting, analyzing, investigatingand controlling HCAIs
- Develop and implement preventive and corrective programs in specific situations where infection hazards exist….
- Review and update hospital infection control policies and proceduresfrom time to time.
HICC shall meet regularly – once a month and as often as required.
Since we’re now 924 days / 30 = ~30 months = 30 meetings into the latest Coronavirus pandemic, one would have expected those regular monthly meetings to have culminated in robust and coherent “politicies and procedures” to prevent the airborne transmission[1] of SARS-CoV2. But who am I kidding? Nothing could be further from the truth.
Here are some revealing anecdotes[2]. (I’m including medical offices because the hospitals are the hegemonic institution in the delivery of health care in the United States, and others could be expected to follow their lead.) For example:
I’m in a hospital right now in Iowa astounded that masks are no longer required. Absolutely bonkers.
— Snickademous (@Snickademous) September 7, 2022
And:
Why am I in a hospital and no one is wearing masks
— Jessica (@jes_klein_) September 8, 2022
Day 2: no masks I’m going to die here
— Jessica (@jes_klein_) September 9, 2022
And:
It does. Was recently in Pennsylvania at a hospital and no masks required. At home in New Jersey, masks required in ALL medical facilities
— Lucy🐾💚 Sadie🐾💛 & Mom 🦄💙 (@corganddox1215) September 10, 2022
And:
My 73 year old brother went by ambulance to an ER in IA cuz he couldn’t breathe. He tested Covid+ & has pneumonia. He was wearing a mask when he got there & staff told him he didn’t have to, IN A HOSPITAL ER! He said one Dr was masked, but no one else. WTH is going on?
— chicky ✍🏻 (@_chicky_little) September 10, 2022
And:
Urgent care last Monday for abdominal pain. Masks optional, people coughing in the waiting room. Wearing my n95. Mammogram today, masks optional in the hospital system. Tech wore a surgical. I was in an n95. Potentially risking my health for urgent and preventative care.
— njphlaz 🐝👩🔬 (@njphlaz) September 9, 2022
And finally:
Dr appt. today, large medical building, lots of dr. offices. Not a single mask on anyone, including my dr and his nurses. I wore my mask.
— Leah Hamilton (@LeaHami55821459) September 10, 2022
At the very least, mask policy — the first layer of defense against aerosol transmission, before ventilation — is inconsistent (or inconsistently enforced) across jurisdictions in hospitals. So it’s no wonder that Politico writes “Nowhere is safe: Record number of patients contracted Covid in the hospital in January“[3]:
More than 3,000 hospitalized patients each week in January had caught Covid sometime during their stay, more than any point of the pandemic, according to U.S. government data analyzed by POLITICO.
The record surge demonstrates the virulence of the Omicron variant and how even hospitals, where infection control is paramount, provided little refuge.
“Any level of hospital transmission is concerning,’ said Aaron Milstone, a professor at the Johns Hopkins Bloomberg School of Public Health who focuses on the prevention of hospital-acquired infections. “The data suggests that hospitals should review their practices and make sure they are doing everything they can to protect patients.”
(lol no.) This article appeared in February, 2022. Six HICC meetings later, nothing has changed. Interestingly, the issue of whether Covid is airborne and if so, what practices to adopt, blew up way back in 2020. From KHN via the Guardian:
Frontline healthcare workers are locked in a heated dispute with many infection control specialists and hospital administrators over how the novel coronavirus is spread – and therefore, what level of protective gear is appropriate.
At issue is the degree to which the virus is airborne – capable of spreading through tiny particles lingering in the air – or primarily transmitted through large, faster-falling droplets from, say, a sneeze or cough. This wonky, seemingly semantic debate has a real-world impact on what sort of protective measures healthcare companies need to take to protect patients and their workers.
In fact, the administrators and the infection control specialists won (as we see from the anecdotes and data above). (See, .e.g., “Some hospitals ask patients, visitors to remove N95s, citing CDC.”) Why?
In this post, I will show that CDC — hold onto your hats, here, folks — rejects airborne tranmission for Hospital Infection Control[4], indeed for Covid. I will then present new data that shows how airborne transmission is pervasive in hospitals, reinforcing the data and anecdotes given above. I will conclude by speculating why CDC is so sickeningly derelict in its mission to “fight disease and support communities and citizens to do the same.” This is especially unfortunate, since the CDC created the field:
Infection control (now infection prevention) in healthcare settings is a relatively young medical discipline dating back only to the 1970s. Nationwide surveillance for healthcare-associated infections (HAIs) was initiated by the Centers for Disease Control and Prevention (CDC) in 1970 via the National Nosocomial Infections Study (NNIS).
Tne CDC Infection Control Documentation Rejects Aerosol Transmission
I’m going to take a short journey through the CDC’s “Infection Control” page, looking for what it has to say about airborne transmission. There is a table of contents at too right; I’ve highlighted the areas I am going to look at:
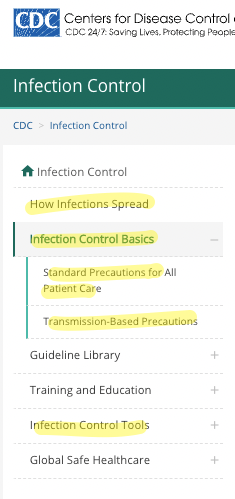
The “How Infections Spread” page has a cute little three-tab widget under the heading “How Do Infections Occur?”. The tabs are “Source,” “Susceptible Person,” and “Transmission.” Let’s look at each tab in turn.
Source;
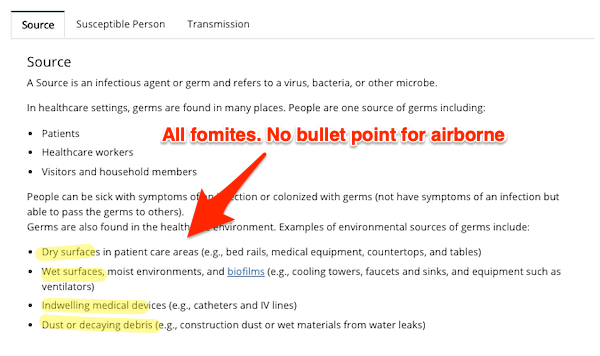
As you can see, this page has bullet points for examples of transmission via fomites, but there is nothing specific for airborne. Yes, “people are one source of germs,” but there is no indication of how or why. One might imagine a bullet point for, say, breathing (which creates shared air). But no.
Susceptible Person:
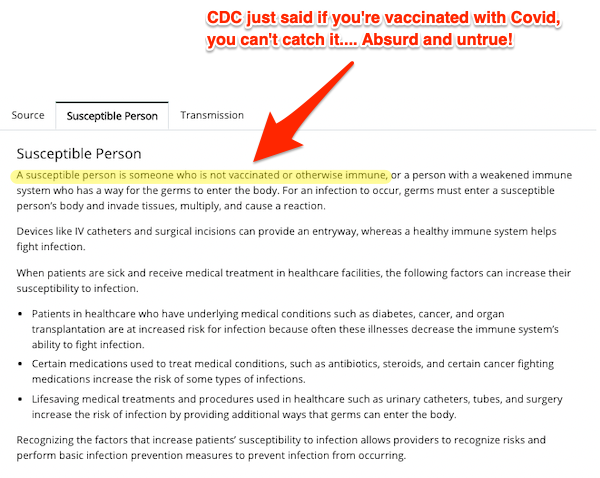
This page contains, at least for Covid, an outright falsehood. Plenty of people who have been vaccinated are “susceptible” to Covid.
Transmission:
![]()
Here, finally, we get a mention for airborne transmission (although one would have expected people to have been given as an example on page one). However, 1) and jaw-droppingly, Covid is not mentioned (which would lead an innocent reader to assume that Covid was not airborne). And 2) aerosol transmission is not confined to “long distance” infection [pounds head on desk]. If you’re sharing air with an infected person, that person can be six inches, six feet, or six yards away (the latter two depending on the quality of ventilation).
Now we turn to the “Infection Control Basics” page. There are two sections: “Standard Precautions for All Patient Care”, and “Transmission-Based Precautions”:
Standard Precautions for All Patient Care:
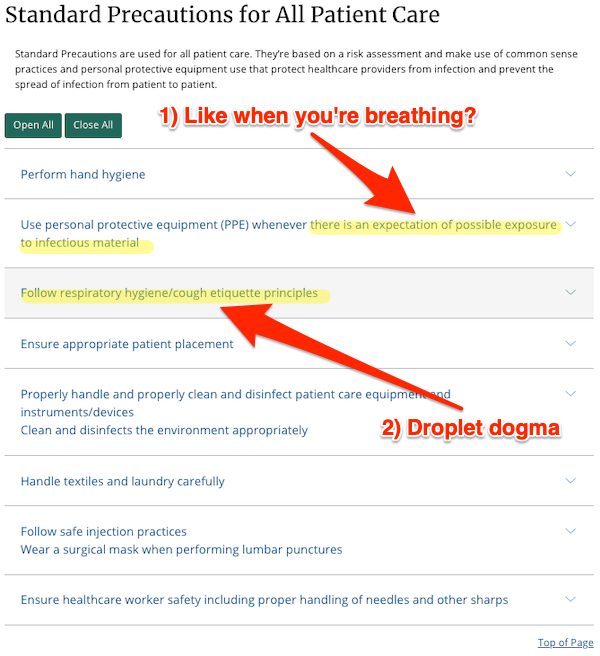
As I shall show below, 1) the possibility of Covid infection in hospitals is pervasive. Hence, the concept that there are some spaces where PPE is appropriate, and some where it is not, is wrong. “Respiratory Hygiene/cough etiquette” 2) is droplet dogma; it ignores airborne transmission via breathing, talking, singing, etc.
Transmission-Based Precautions
![]()
Once again, 1) there is no mention of Covid. A reasonable reader, considering the salience of Covid on the nightly news or in professional literature, would conclude that Covid is not airborne. 2) The idea that infectious/susceptible persons should be given separate rooms flies in the face that the fact that airborne Covid is pervasive in the hospital setting. Meanwhile, the idea that one might 3) place them in a separate room, but without a HEPA filter, is absurd.
Finally, we turn to the page for “Tools for Healthcare Settings.” (If you go to the link, you will see that there is nothing specific for airborne transmission)
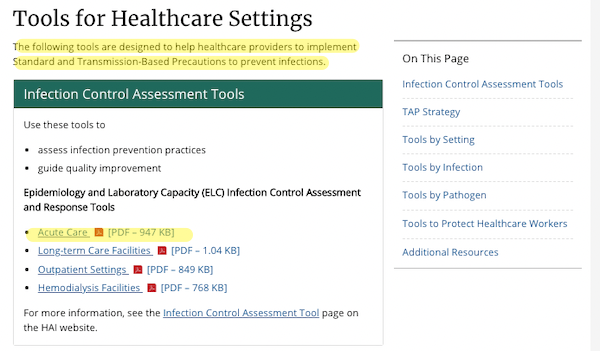
I will look at the “tool” for “Acute Care,” which I take to cover hospitals.The “tool” is in fact a ginormous survey instrument (PDF). Here is the heading:

“Assist in the assessment of some infection control programs” this “tool” certainly does. But I can assure you that there are no entries for “ventilation,” “HEPA,” or anything useful for “air.”
There is an optional section that mentions “airborne,” I suppose on the assumption that only some facilities have issues with airborne transmission of Covid:
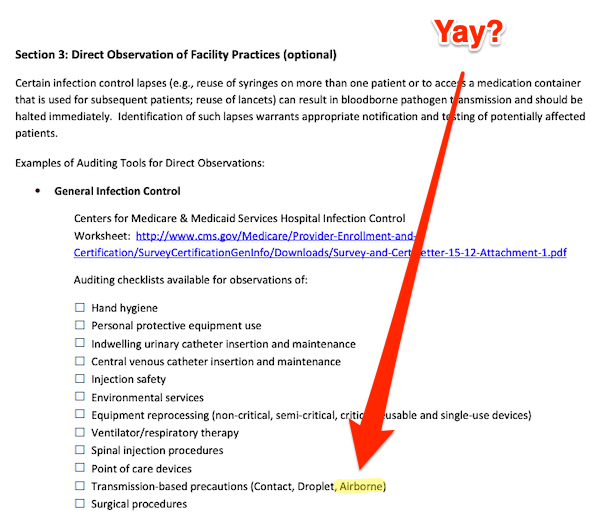
So I clicked through to the link given, and found a “Hospital Infection Control Worksheet” from CMMS. Here is the first page, but the rest has the same assumptions:
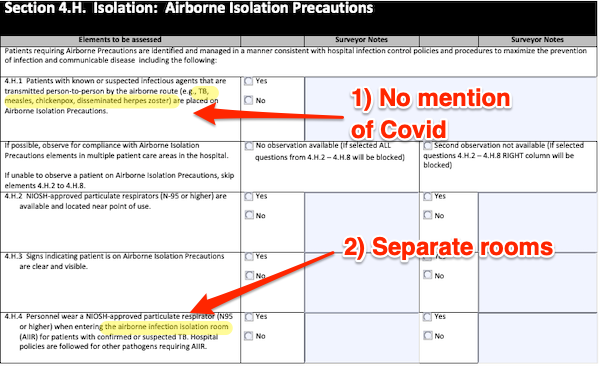
So we find the same weaknesses as in “Transmission-Based Precautions” above. 1) Covid is not mentioned. 2) Infectious Persons are to be placed in AIIRs (Airborne Isolation Infection Rooms) in which, in section 4.H.6 on the next page, and contradicting earlier guidance, HEPA filters are mandated, just not for everyone else. So there’s no thought of HEPA filters anywhere else, like ordinary rooms, or waiting rooms, or offices.
A reasonable person would conclude from reading this checklist that if a hospital can isolate measles patients, it can handle airborne transmission in the general case. Not so!
So if you’re looking for a reason why HICCs keep meeting, month after month, and not accepting that Covid is airborne, or doing anything about it, it’s because their hegemonic authority on infection control, CDC, hasn’t given them any reason to believe otherwise. For starters.
Airborne Transmission of Covid is Pervasive in Hospitals
From the preprint “The aerobiology of SARS-CoV-2 in UK hospitals and the impact of aerosol generating procedures“:
Aerosol generating procedures (AGPs) seemed particularly risky, and policies have restricted their use in all settings. We examined the prevalence of aerosolized SARS-CoV-2 in the rooms of COVID-19 patients requiring AGP or supplemental oxygen compared to those on room air.
(An example of an AGP is a tracheotomy. AGPs are the only form of aersols in hospitals that “droplet dogma” permits.) From samples in 219 rooms, ” the largest air sampling study for SARS-Cov-2 published to date”:
SARS-CoV-2 viral RNA was detected in the air of hospital rooms of COVID-19 patients, and AGPs did not appear to impact the likelihood of viral RNA. Enhanced respiratory protection and appropriate infection prevention and control measures are required to be fully and carefully implemented for all COVID-19 patients to reduce risk of aerosol transmission./
And concluding:
Appropriate PPE and mask use are essential as SARS-CoV-2 is frequently detectable in the airsurrounding positive patients. We believe our data supports the use of FFP2/3 medical masks for HCWs caring for COVID-19 patients, particularly for those with prolonged contact in line with HSE guidelines 15 289 . As we move forwards, we must continue to avoid oversimplifying the transmission dynamics of SARS-CoV-2 including into ‘droplet vs aerosol’, as this can lead to fixed IPC recommendations and must now appreciate that the ‘person, place and procedure’ influence transmission risk. Future recommendations must be guided by emerging evidence including ongoing studies to identify transmission differences that may occur with new variants of concern
In other words, Covid is pervasive, rather like background radiation. Covid really is airborne!
Conclusion
One asks why? Why would CDC promulgate, and HICCs accept, obvious falsehoods about airborne transmission, falsehoods that are obvious to anybody who keeps up with the literature? A parallel discussion of CDC’s documentation on ventilation in schools may provide a clue.
A week ago, I had a 2+ hour call with the senior engineers from CDC-NIOSH who are responsible for the content of CDC’s ventilation pages.(12/25)
— Devabhaktuni “Sri” Srikrishna (@sri_srikrishna) September 11, 2022
ACH (Air Changes for Hour) is a metric for ventilation:
(2) economic implications of putting these ACH numbers out there would cause “all hell to break loose” if well-meaning people across the country adopt them into building codes but later find out they cannot implement them with centralized HVAC systems. (16/25)
— Devabhaktuni “Sri” Srikrishna (@sri_srikrishna) September 11, 2022
Money! [slaps forehead][5]. Why didn’t I think of that? Also, of course, careerism, important to the PMC. So here we are.
NOTES
[1] Covid’s Most Vile Tweet™ is still up [pounds head on desk]:
FACT: #COVID19 is NOT airborne.
The #coronavirus is mainly transmitted through droplets generated when an infected person coughs, sneezes or speaks.
To protect yourself:
-keep 1m distance from others
-disinfect surfaces frequently
-wash/rub your 👐
-avoid touching your 👀👃👄 pic.twitter.com/fpkcpHAJx7— World Health Organization (WHO) (@WHO) March 28, 2020
4,340 quote-tweets, the last one fourteen minutes ago (as of this writing). So WHO is still damaging people’s health, good job,
[2] The United States seems, unbelievably, to be superior in mask protections to other “Five Eyes” countries, like the UK, Canada, and Australia, if the volume of outraged tweets is any indicator. Of course, in the US we may have just given up on outrage altogether, as with Covid generally.
[3] In the UK: “Transmission of SARS-CoV-2 to hospitalised patients likely caused approximately a fifth of identified cases of hospitalised COVID-19 in the “first wave” in England, but less than 1% of all infections in England.”
[4] The UK infection control community is as bad and possibly worse.
[5] I suggested the same in February 2021, based only on CDC documents [lambert preens].
APPENDIX: If Your Heatlh Care Facility Forces You to Remove Your N95
If you do not carry a Badger Frame (or Seal), here is a post on “How to Make a DIY N95 Mask” using a surgical mask and two eight-inch rubber bands.


I have filed several public information requests regarding use of American Rescue Plan funds for ventilation in schools and public buildings.
I have found some very interesting information that I hope to post soon. I am still waiting for some additional info.
Any tips on how to file these?
Go to the website for your municipality, school district, community college, and university and search for “Public Information Request”.
There should be directions on how to file. I have found that some take email requests, fax, snail mail, or walk in drop off requests.
Be aware that they can charge you for copying, research time, etc.
Be specific. In my requests, I asked:
Did the municipality, school district, community college, university use ARP (American Rescue Plan) funds to improve air quality? If so, how much was spent on improving air quality? What were the funds used for?
After I got those answers, I filed followup requests, because there was some info that came out in their original replies.
Based on some of the replies, I need to file requests with the state education agency because they were responsible for approving HVAC requests.
I am still in the process of collecting info.
In the height of the pandemic, I lived in a collective with 90 other artists in East London in a decommissioned Salvation Army hostel.
Almost immediately as information about Covid became available, we instituted policies and protocols based on SARS and MERS. Unlike most communal living situations, we had NO endogenous CV-19 cases.
The hostel was specifically designed to minimize air flow, and no matter how much scientific research I threw at the property manager showing that the cheapest and most effective way to reduce CV-19 transmission was to maximize air flow by keeping as many windows and doors open as much as possible, they insisted on keeping all doors and windows closed with a zealotry worthy of Oliver Cromwell.
Ultimately, I escalated the dispute to the London Fire Brigade, going so far as to hand deliver pages of research to the Fire Brigade Commissioner.
Their response? Regulations are regulations.
It did not matter that in all of the UK in 2019, there were 262 fire-deaths vs. 130,000 CV-19 deaths as of that point.
If I wanted to keep the doors and windows open, the regulations would have to be changed.
The second most effective way to destroying aerosol transmission iof CV-19 is UV-C air sanitizers.
The NHS never gave them a second thought, whereas TFL (Transport for London) installed them in their Underground stations. A huge number of people I know actually contracted CV-19 in NHS hospitals and waiting rooms. Can’t say about the people who might have caught it on the Underground. But what is the world coming to when it is safer to travel on the Underground that go to an NHS hospital?!
A friend who works for the NHS explained that the TFL is actually not a government entity and can make rapid decisions like purchasing UV-C air sanitizers. (A fact I didn’t know). The NHS is a huge bureaucracy, and by the time all the testing, writing specs, putting out tenders, purchasing and distributing the sanitizers was complement, the pandemic would be over.
Even if, as it turns out, this was not the case.
Very much looking forward to the result!
https://www.cbsnews.com/news/model-architecture-serving-society-60-minutes-2022-09-04/
The MASS model of community-focused architecture
Video and transcript at the link.
…
From Wired, May 2021, https://www.wired.com/story/the-teeny-tiny-scientific-screwup-that-helped-covid-kill
I.e. it’s all about the Benjamins.
This is a real public service. Interestingly, there’s a web page annotation service that lets you annotate pages and these can be shared with others. It would be both hilarious and instructive if someone had corrected the CDC’s murderous inaccuracies. Sadly a search doesn’t bring up any evidence that this has been done.
Which is to say, right where we’ve been all along, since before the germ theory or any of the rest of the concepts and methods of modern medicine. Our fundamental problem is with how power is structured and influence exerted.
Some years ago someone at NC, in my recollection it was you Lambert, posted some writings by a fellow who (circa 1900 I think) used little more than a very astute appreciation of the world as it was then, and the assumption that those with power will act in their own, unenlightened, self-perceived, short-term interests, and wrote a remarkable, almost prescient, forecast of things to come. I remember thinking that his success meant we were probably going to be screwed to the wall by global warming.
Pestilence actively promoted by the rulers didn’t even enter my thoughts.
This is an obscene betrayal of trust on the part of the CDC and WHO.
I do wonder how much it cost in terms of time ( You don’t fully corrupt an agency overnight) and money.
For most involved the reward is no more than keeping their job with its nice benefits.
Some will make a few bucks, I’d be surprised to find out Fauci hasn’t.
No one made a killing financially except big pharma.
Just a Million and change actually dead, hundreds more dying daily and an unknown number ( In the Millions) afflicted with Long Covid.
I doubt any of those who are going along to get along have made more than a few pennies for each death.
Life is cheap in the USA, Living is not.
Masks aren’t the problem. Following protocol is.
If IM Doc is reading this post, I’m certain he can attest. During COVID, kid #2 had to have “routine” surgery. A screw that was implanted was contaminated (tested positive upon removal). Kid #2 ended up contracting pseudomonas aeruginosa, in the middle of COVID. COVID was not even an issue, as the infectious disease doc told us “treatment” will or won’t work. Those were the outcomes.
So yea, please save your masks. Good grief.
I had a stroke back in 2015. I spent 5 days in the Cardiothoracic ICU (no room in the Neuro ICU), where heart transplant patients are cared for, and 5 in a room in unit where all the other patients had contagious conditions that required staff and visitors to wear protective gear. I couldn’t believe how dirty everything seemed. After I got home I asked my wife if that was an accurate perception and she said it suprised her too – not what she remembered from when we were younger.
Hospitals in the US should have much much better ventilation, but I wonder how many are just plain dirty?
It does not have to be this way. When I got my titanium hips at the Hospital for Special Surgery, I saw how they were anti-infection fetishists. Not only was everything clean…..in operating theater, the surgeons and attending nurses do not breathe the air in the room. They wear masks that have them breathing outside air.
I think the White House has also decided that the key to electoral bliss is to declare victory and sweep COVID under the rug. Can’t have things like people in masks or attention paid to ventilation. Spoils the optics.
As Joe Biden’s mentor Donald Trump said early in the pandemic, “if you don’t do the testing you won’t have the cases.” The Democrats basically stole Trump’s Covid policy, but without the Operation Warp Speed money for updated vaccines.
I will be attending via Zoom
Justin Feldman, ScD “How to Hide a Plague: How Elite Capture and Individualism Made Covid Normal”
Date & Time Sep 22, 2022 12:00 PM Central Time (US and Canada)
Webinar ID 977 2021 9283
Passcode 019257
You can register at
https://www.utmb.edu/ibhh/news-events/events-single-listings/2022/09/22/default-calendar/september-22-2022
Yeah, that paragraph alone was very satisfying to read, so I signed up. I’m not sure to what extent Feldman is pro-TTIQ/containment/elimination/the dreaded L-word* but he really does seem to get it, and that paragraph is rhetorically similar to GM’s arguments that we’ve seen here the last couple of years.
* by way of comparison, the excellent @wsbgnl has a great grasp of a lot of Covid’s political issues but, while he does defend China’s deliberately non-homicidal, non-disabling policy, he does pull his punches about whether containment is worth doing or can be done, remembering the question of whether it can be done has to be subdivided into the question of whether it can be done technically – which it can, pretty straightforwardly – and whether it can be done politically – which it can’t, not because to do so would be tyrannical unfreedom, but because of the entrenched power of extremist capitalist fanatics in the western world. The answer to the political question, of course, is and always will be mutable. But it will require us to rather get our shit together.
I will be interested to hear your report :-)
I just QT’d that horrible WHO Tweet. Now at 4342.
Here’s what the inception planted in the minds of the many:
• COVID isn’t really airborne – I only have to worry is someone is coughing or sneezing next to me.
• People can only transmit COVID if they are discernibly sick and have symptoms, so if someone doesn’t have symptoms, they can’t give me COVID.
• COVID is mild if you’re vaccinated, so even if you get COVID, the vax will protect you from serious illness.
I see it everyday. Saw it today. Only person masked in the one store I went to at a mall. One of few masked at the grocery. But yes, it’s disheartening to see so called health care professionals doing this.
Just caught up with this post and it was as bad as I thought it would be. Exasperating does not even come close to describe those tweets. These policies may have been both explainable and forgivable in mid-2020 but not now. Not two years later. So I will change the title of this post to a more correct wording that we normally see and would have it so-
‘Hospital Infection Control Departments Tenaciously Resist Airborne Transmission, Aided and Abetted by CDC’
I continue to believe that CDC and WHO try to let it look like its “all about the money” so as to escape scrutiny over the possibility that it is really about “killing as many millions of people as possible short of being caught red handed killing as many millions of people as possible”.
I continue to believe that mass democide is the CDC goal. Any money saved is just gravy.
> mass democide is the CDC goal. Any money saved is just gravy
One hand washes the other. If eugenics* weren’t profitable, we wouldn’t be doing it.
NOTE * I have settled on eugenics as opposed to either “social murder” or democide, because I think most people don’t need to have the term explained to them, and they know it’s very bad. (I think at some point I will be able to nail down actual eugenic ideology/intellectual history among the ruling class, the 1%, using anti-vax ideology as an entry point. We shall see.)
How to square with ruling class itself also at risk of bad outcomes? Perhaps they simply don’t believe long-COVID or progressive vascular and neurological damage manifest? If death is the only relevant endpoint to acknowledge or avoid, then they’re sitting rather pretty right now whereas social undesirables, not so much.
This all seems a bit like an own goal though.
This problem occurred to me also. “Eugenics” may end up being the only already-known word to apply to the elites’ time-delay mass-murder policy. But since they, including their scientists, all gather together in unmasked unventilated super-spreading events and super-spreading venues; the word “eugenics” does not quite describe the suicide death-cult nature of their own behavior.
Generally speaking, I think the roots of this mask resistance in non-Asian countries – particularly those who hadn’t completely politicised masking in the first place in the most hopelessly braindead fashion like the United States – in large part comes down to the carrot/stick approach of encouraging vaccination. The carrot was the promise of abandoning masks. The stick was mandates (applied to varying degrees around the world, mostly abandoned now that everyone intuitively understands how lame the vaccines are even if they don’t want to come out and say it).
If the vaccines had been capable of single-handedly ending SARS2, then I’d argue that would be fair enough. But they never were (and the extent to which people were misled about this being possible really does remain fairly mind-boggling).
But for the most part, people did what they were told and expected to be commensurately rewarded, ie with the promise of removing masks, aka “The Scarlet Letter of the Pandemic” (Walensky) because they were told the pandemic was over, and are now told that we have the tools (but not masking, which is apparently a tool of the “you do you” variety, which some might argue is the perfect summation of a selfish culture and/or era).
So this incoherent stew of public health quarter-measures has led us to a point where rampant nosocomial infection is simply shrugged off, because we seem to be in the most profound denialist stupor: that of the dickheads that claimed SC2 was never a big deal in the first place, and that of the dickheads who are committed to pretending that we live in the best of all possible worlds.
Thanks as ever to Lambert for another robust write-up.
Ultimately, its been a gigantic failure in public communication.
I’ve watched here in Ireland how the health authorities did a pretty good job at the beginning in sending out clear messages (albeit with far too heavy an emphasis on fomites). But it slowly disintegrated over 2 years into absolute incoherence. Nobody has any idea what the official message is, so everyone just ignores occasional pleas to wear masks. A colleague recently asked me why I’m still masking – she seemed genuinely puzzled, not hostile.
It is not just in western countries – Naomi Wu has been tweeting recently that the Chinese authorities have been very poor at communicating with people why they are doing what they are doing (she has pointed out that historically public health messaging is one thing the CCP was very good at), and even in Japan the message is getting very muddled. While in western countries the messaging seems to be getting more incoherent and worthless, in Asia its devolving into ‘just do what we tell you and don’t ask any stupid questions’.
This really is a brain rotting virus.
> The carrot was the promise of abandoning masks. The stick was mandates
I don’t think your timeline is quite correct. The idiotic idea of using unmasking as a stick came long after the initial message-butchering by WHO, the Centers for Disease, and Fauci.
Trump and his supporters deserve their fair share of credit for anti-masking. Trump made ” no mask” a symbol of personal freedom and personal manhood through such stunts as refusing to wear a mask when photo-opp touring a Ford plant. Large numbers of Trump supporters bragged about their superior personal manhood and freedom-hood by not wearing masks.
Pro-Trump terrorist mobs obstructed mask-mandate applications in various states, including Michigan. Pro-disease Trump supporters made mask-mandating and other public health measures so dangerous to try applying in Michigan that no Michigan government will try responding with public health measures to public health emergencies ever again. Pro-Trump bug-spreaders have driven public health officials out of their jobs in several jurisdictions here and there.
It is disingenuous to withhold from the Trumpers their fair share of the credit for anti-mask-ism in America today. Believing the only danger comes from the PMC Democrats puts the believer at personal risk from every Typhoid MAGA coronavid plague-spreader the believer is unfortunate enough to have to share infected air with.
Excellent article — bookmarked!
My wife was in the hospital because of a broken leg bone. In talking with her doctor about being discharged, the doctor said he wanted to get her out of the hospital as soon as possible.He said the hospital is the worst place to be because of the threat of being infected.This was a surgeon that had practiced for over 20 years in our area.
the hospital is the worst place to be because of the threat of being infected
to be fair, hospitals have been dangerous places for this reason for as long as they have existed – it’s not just now – but maybe it is even more risky during a time of pandemic, admittedly
Stuff like this is why I haven’t been to a doc in almost three years.
I know a doctor who is shortly going on a cruise. In the Mediterranean. Requiring her to fly there first with her toddler. This kind of behavior is normal for doctors right now.
I’ve also heard that there is a higher proportion of sadists in doctor populations. No ref for that and I’m still inclined to believe.
It’s one of the many taboo subjects in our society, but the helping professions can offer people with sadistic tendencies both opportunity to indulge their impulses and cover for their motives.
I saw an interview with Michael Hudson where, speaking of Madeleine Albright, he said something to the effect of “She just wanted to hurt children.” I think of that every time I read the latest from Leanna Wen or that British pediatrician, whose name eludes me at the moment.
Quite an accusation without a reference. Hope you stay healthy.
Thank you for this post. Sad that NC is one of the few media sources I can find still taking an anti-covid stance in 2022. I just made a donation to the fundraiser, as NC serves an important mental health function at this point in the pandemic – by reminding me that I’m not actually nuts.
As other comments have mentioned, this is the reason I have avoided any medical care throughout the pandemic. I did go get a physical in the lull between when the first vaccines became available but before Delta, Omicron, and the other variants emerged. The doctor and nurse practitioner who saw me were just wearing surgical masks. The receptionist had her’s below her nose. This was before masking had been 100% abandoned by authorities and the public, but the necessity of N95 masks was already established. I did wonder how I was supposed to trust any doctor who couldn’t be bothered with this relatively simple precaution, in the middle of a pandemic of an airborne respiratory virus. It’s maddening.
local anecdotes–sorry this got so long–
my local hospital is in a small town in a rural state in the northeast. mask wearing is still required for patients and staff. most staff wear surgical masks. there are plexiglass barriers in places where workers encounter a steady stream of people checking in. i have not had the energy or time to try to find out what they are doing with ventilation.
i was there today for a stereotactic biopsy, done with the aid of mammography.
i had asked in advance if all involved could wear N95s and this was agreed.
the dr. arrived wearing an elastomeric.
the others were wearing N95s. (the biopsy went well.)
however, on my way in i had to register. you sit at a desk behind which is a staff member at a computer, in front of which hangs a plexiglass barrier (i think–i may not remember accurately). today that person was receiving training.
she told me (in response to my questions):
she is being taught how to do various jobs around the hospital, because many staff are leaving.
she said that is not new, but with people expecting the next round of covid coming in the fall and winter, there’s been more of it.
she said it’s basically because they are required to get the latest vaccination and they are not willing to.
clearly, they know what we at NC know about this latest vacc.–no guarantee it’s effective, possible side effects, very short term even if effective at all.
she also told me that she has long covid.
she got it in january. her symptoms include bone pain and occasional really bad headaches, and more that she did not want to go into. she said it is really bad. her doctor is doing everything he can to run tests and try to find ways to help. he is sending her to a neurologist.
she also said that she’s been urged to stop coming to work, but she loves working and would rather come in.
the other day i walked my dog with a new acquaintance. she told me that her young son had started to get bad headaches, which at first she thought were nothing to worry about. until during one of these headaches he started vomiting. after interviewing him at length, the pediatrician told her that children normally do not get headaches at night, as he has been. he is going to see a neurologist. she brushed off my question whether she thought it might be covid related–i suspect simply feeling that knowing that it was long covid would not help her to navigate the process of his care any more easily.
meanwhile, since may, my 90yo partner has been in a nursing home in another part of the state. perhaps i will report more here some time on the covid situation there and the problems in elder care here (and everywhere, i’m told) arising from health care workers’ massive exodus.
what i had not fully understood until today’s conversation at registration and now feel i do (i could be wrong) is that many of them understand quite well the covid risks they undergo in health care settings, they understand the bullshit and the inadequacy of the protections they’ve been provided, they’ve never really bought into the vaccination hype, and they are deciding not to risk their lives or future functioning if they can find a way to avoid it. but if all this is true, i still do not understand why those who choose to/have to continue to work in these settings do not choose to wear N95s at work.
correct me if i’m wrong, but i feel like i’m not specifically seeing this massive exodus discussed much as what it seems to me could be the most dire of all the outcomes of the failure of the administration of responsible public health measures for covid. but the effect on quality of all medical care across the board must be noted. if your hospital room seems dirty, that is probably because it has in fact not been cleaned. if hospitals always have been a bit of a risk for bringing home a bug you do not want, they are now or will soon become disease vectors at a level beyond anything most of us now alive have experienced in the USA. it is not hard to guess why this disaster across the nation’s entire medical system has not been widely described in its full horror. thanks to all at NC for making the effort to do so.
one of the things that has been heartbreaking is witnessing how caring and responsible are so many of the staff who continue to show up.
> health care workers’ massive exodus
It’s not a problem. The rich will always get health care. The PMC will believe they can, by doing their homework, and will not believe they cannot until it’s too late.
Need to watch the media for stories about robots in hospitals…
Airborne protection in hospitals is based on the low prevalence of tuberculosis.
There have never been enough negative air pressure rooms for COVID, and a quick web search shows companies are trying to fill the void.
Failure to fund this upgrade is one of the lesser renowned public health debacles. Still not happening…
> There have never been enough negative air pressure rooms for COVID, and a quick web search shows companies are trying to fill the void.
If they are, that is IMNSHO the wrong approach. The air in the entire hospital needs to be cleaned. the infection control paradigm in my view is very spatially oriented; they think they can wall of a particular area and make it safe; hence the frankly risible fudge of “Aerosol Generating Procedures.” They just bite the bullet and put HEPA machines everywhere, if the HVAC systems cannot be made to do infection control (authorities differ on this, so I need to do more research on what is really possible).
Part of a New Green Health Deal could involve spending as many billions of dollars as necessary improving the ventilation of buildings up to covid stopping standards as is necessary to stop spreading covid in buildings.
That could be something a New Green Health Deal Party could run on to see if it gains brainshare among the public.