By Lambert Strether of Corrente.
As readers know, I stan for Covid nasal sprays, whether as prophylactics or vaccines (see here and here, plus many mentions in Links and Water Cooler). So I figured it was time for another look, because “science is popping.” I should say right away that the headline is a bit deceptive. The elephant in the room is that India’s Bharat Biotech, a major contract vaccine manufacturer, will be launching its own nasal vaccine, iNCOVACC (BBV154), tomorrow, January 26, on Republic Day. However, that story has so many imponderables — including, last I checked, missing clinical trial results in journals where I would expect to find them — that I feel it deserves a post of its own when matters are a bit more sorted.
Here is the problem statement. This is the problem that nasal vaccines are meant to solve (and nasal prophylactics to ameliorate). From Cell (pre-proof), “Upper respiratory tract mucosal immunity for SARS-CoV-2“:
Early control of SARS-CoV-2 infection and prevention of transmission are heavily dependent on robust mucosal immune responses in the upper respiratory tract (URT). However, current licenced SARSCoV-2 vaccines induce predominantly systemic responses, rather than potent, durable responses in the URT mucosa. Thus, despite their effectiveness in reducing disease severity, hospitalisation rates and mortality, these vaccines do not generate sterilising immunity, thereby having a limited role in preventing infection and blocking subsequent viral transmission. Suboptimal vaccine-induced immunity that does not adequately inhibit transmission in the community, hence permitting ongoing cycles of viral replication, can promote the establishment of new, highly virulent, vaccine-resistant SARS-CoV-2 variants. Although current licenced vaccines may be effective against severe disease and death, even if to variable degrees, against some SARS-CoV-2 variants of concern (VOC), the VOC demonstrate an aptitude for immune escape with significantly reduced sensitivity to antibody neutralisation. Further, while Omicron-adapted bivalent vaccines can increase the breadth of neutralisation of different SARS-CoV-2 strains systemically, suggesting this approach may mitigate the impact of Omicron BA.4/5 as well as new emergent VOC, transmission cannot be prevented without the induction of URT mucosal responses.
Which pretty much describes where we are, doesn’t it? And where we would like to be. Indeed, it’s an exciting time to be a mucosal immune response enthusiast! The most interesting and encouraging news is that we now have a mechanism for how Covid — which is airborne, needless to say — infects the body through the nose, and to that I now turn.
The Science: SARS-CoV-2 Infects Us Through the Nose
December 2022 and especially January 2023 saw a drumfire of publications on what a layperson would call nasal infection (or, as we like to say, “replication in airway epithelia”). This article in Cell by Wu et al. (noted in Water Cooler on January 10) was especially impressive:
Using primary nasal epithelial organoid cultures, we found that the virus attaches to motile cilia via the ACE2 receptor. SARS-CoV-2 traverses the mucus layer, using motile cilia as tracks to access the cell body. Depleting cilia blocks infection for SARS-CoV-2 and other respiratory viruses. SARS-CoV-2 progeny attach to airway microvilli 24 h post-infection and trigger formation of apically extended and highly branched microvilli that organize viral egress from the microvilli back into the mucus layer, supporting a model of virus dispersion throughout airway tissue via mucociliary transport. Importantly, Omicron variants bind with higher affinity to motile cilia and show accelerated viral entry. Our work suggests that motile cilia, microvilli, and mucociliary-dependent mucus flow are critical for efficient virus replication in nasal epithelia.
(Note that “24 h post-infection” which will become important later.) Here is a graphical abstract that illustrates the process of infection:
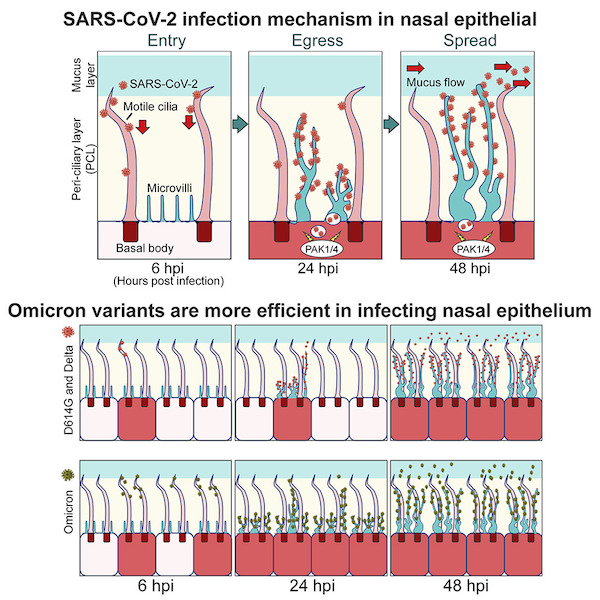
This is important because at long last we have a mechanism of infection; now we can say not only that “covid is airborne,” we can trace its path into the body (which presumably will be of great help to all the vaccine developers out there). To translate Cell into English, “Scientists pinpoint the routes taken by SARS-CoV-2 to enter and exit cells in our nasal cavity” explains the ingenious and fascinating laboratory techniques Wu et al used, all well worth a read, and concludes:
The findings identify new targets for a nasally applied drug that, by impeding ciliary motion or microvilli gigantism, could prevent even unknown respiratory viruses — the kind you meet, say, at a pandemic — from making themselves at home in your nose or throat.
[Co-author Peter] Jackson said substances used in these experiments could perhaps be optimized for use in, say, nasal sprays soon after a respiratory viral exposure, or as prophylactics.
“Delaying viral entry, exit or spread with a locally applied, short-duration drug would help our immune systems catch up and arrive in time to stop full-blown infection and hopefully limit future pandemics,” he said.
(Note that Jackson’s vision for a “nasally applied drug” does not include vaccines, nor does the Stanford press release describing the work; but that may be product-driven; although a “morning after” nasal spray sounds like a good idea.)
However, a mechanism for nasal infection raises the possibility of a “sterilizing vaccine”[1], in essence eliminating the necessity for both CDC’s “red map” and its “green map” (as well as regular injections into muscle). From The Mail, in January 2023:
Muhammad Munir, a professor in virology and viral zoonoses at Lancaster University, believes nasal vaccines offer a solution as they ‘halt community transmission’ — in other words, stop people getting ill with Covid and passing it on.
Professor Munir says that’s because Covid enters the body via infected droplets [sic] hat gain entry mainly through the nose or mouth, the logical approach is to focus the immunological fight there. As he explains, vaccines given into the arm produce T-cells (which knock out infected cells) and B-cells (which produce antibodies that attack invading pathogens).
‘But these immune cells are predominantly in the bloodstream and organs, with only a tiny quantity in the nose and mouth so they aren’t guarding the point of entry.
‘And yet for Covid the route of transmission is through the nose and mouth. This area is lined by a mucus membrane that continues to the gut and is enriched with an armoury of immune cells.
‘If a vaccine is inhaled or given as drops through the nose or mouth then it will prime these cells, which are the first line of defence, to act quickly.’
And now comes the “24 h” part–
T-cells and B-cells in the mucosal layer can prompt a lightning-fast attack ‘pretty much the instant the virus comes in’, attacking it before it has a chance to infect cells, he says. ‘These nasal immune cells get to work in a couple of minutes — whereas the immune cells made by intramuscular vaccines get to work six to eight hours after entry of the virus.’
This time difference, he says, is vital. ‘If just one virus particle successfully sticks to one cell it takes over that cell and replicates to produce a million more viruses in an eight-hour cycle,’ says Professor Munir, who has been leading the research into Lancaster University’s nasal vaccine.
‘That’s why the nasal vaccine will have the advantage — the immune cells it produces in the nasopharyngeal region can act immediately. It’s a bit like having the police sitting and waiting for a crime to be committed.
‘With the intramuscular vaccine approach, the police only come once the problem is there, and by that time damage could be done.’
However, it would only be fair to say that nasal vaccines face challenges. From Cell, also in January 2023, “Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses“:
Past unsuccessful attempts to elicit solid protection against mucosal respiratory viruses and to control the deadly outbreaks and pandemics they cause have been a scientific and public health failure that must be urgently addressed. We are excited and invigorated that many investigators and collaborative groups are rethinking, from the ground up, all of our past assumptions and approaches to preventing important respiratory viral diseases and working to find bold new paths forward.
Here is a table summarizing these challenges:
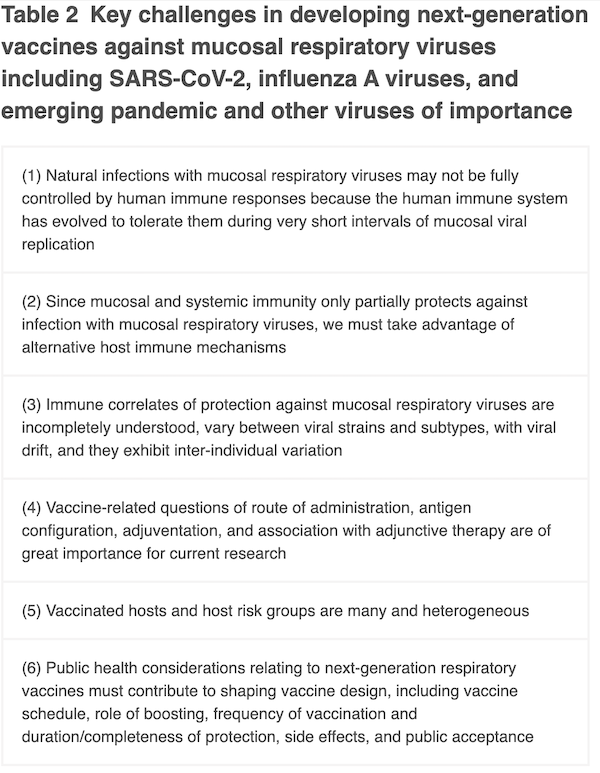
They conclude:
Taking all of these factors into account, it is not surprising that none of the predominantly mucosal respiratory viruses have ever been effectively controlled by vaccines. This observation raises a question of fundamental importance: if natural mucosal respiratory virus infections do not elicit complete and long-term protective immunity against reinfection, how can we expect vaccines, especially systemically administered non-replicating vaccines, to do so? This is a major challenge for future vaccine development, and overcoming it is critical as we work to develop “next-generation” vaccines.
Harsh, but fair. Of all the points, I will address only #4 (“Vaccine-related questions of route of administration, antigen configuration, adjuventation, and association with adjunctive therapy are of great importance in current research”). I would also remind readers that engineering advances can happen before science comes along to back them up.
Advances in Nasal Vaccine Administration
Here too the science is popping. Another article from January 2023, in Nature, “Biomaterials for intranasal and inhaled vaccine delivery“:
Once administered, respiratory vaccine formulations need to overcome various airway barriers to achieve protection (Fig. 1). The mucus lining the airway acts as a semi-permeable barrier to inhaled materials, and foreign material is usually rapidly cleared by motile cilia on the epithelial surface of the respiratory tract. Depending on their size and surface chemistry, vaccine nanoformulations consisting of nucleic acids, lipids, polymers, proteins and/or entire viruses can be trapped within mucus following inhalation. For example, adenoviral vectors used in the development of vaccines against SARS-CoV-2, HIV and tuberculosis can adhere to mucus, limiting the ability of the virus to reach target cells (for example, pulmonary dendritic cells) to elicit robust mucosal immune responses. Non-viral vaccine platforms, such as lipid-based mRNA vaccines, can be designed to overcome the mucus barrier, and may thus allow respiratory vaccination. For example, an inhaled nanoparticle vaccine coated with polyethylene glycol (PEG) can rapidly penetrate the mucus barrier and enhance the proliferation of antigen-specific T cells in the lungs and lymph nodes, as compared with intramuscular delivery of a carrier free vaccine.
So, now that we know that understanding mucus is important, we’re understanding it.
Poor Clinical Trial Results are Said to Be a Barrier
From CBS, “COVID-19 vaccines: From nasal drops to a redesign, what 2023 could have in store“:
A few of these vaccines have been licensed in other countries, but none in the U.S. — and the data behind them isn’t robust, said Dr. John Beigel, associate director for clinical research at the National Institute of Allergy and Infectious Diseases.
Even if Congress had granted the Biden administration’s request to pour resources into developing potential next-generation mucosal vaccines to broad clinical trials, Beigel said it would be challenging to “pick the winners” for government backing. .
Different companies have researched mucosal vaccines for COVID, but the data is small and fragmented, Beigel said, using different methods and benchmarks. This makes it difficult for scientists to compare early results from labs that have tried out new vaccines in animals.
“It is also not at all clear from well-controlled clinical trials that administering existing vaccines by the intranasal route (as some countries have already even approved) will provide truly meaningful benefit over the existing generation,” wrote the authors of a viewpoint co-authored last month by Dr. Peter Marks, the FDA’s top vaccines official.
All of which argues for, at a minimum, funding — and at a maximum, a second Operation Warp Speed, as advocated by Eric Topol here. I mean, asking Pfizer, Moderna, or AstraZenaca to invest in a nasal vaccine that could be sterilizing — instead of demanding endless rounds of injections by trained personnel at medical facilities — is a bit like asking Gillette to engineer a self-sharpening razor blade suitable for lifetime use, isn’t it?[2]
Conclusion
Eric Topol wrote in 2021:
I still cannot understand why intranasal vaccines have not been given top priority, given their remarkable allure to block Covid transmission; an excellent explainer for why and status @ScienceMagazine https://t.co/2T3cFElaXY
w/@ScienceVisuals pic.twitter.com/6VHG90kbc8— Eric Topol (@EricTopol) July 26, 2021
And in 2022:
[Topol] said nasal vaccines are our best shot to block infections. Those spray vaccines are effective in the very place where virus-laden aerosols enter the body. They’re already being used in India and China.
“I’m confident we will have nasal vaccines that work. The only question is, do they work for a few months or is it longer,” Topol said. “It should work against all of the variants. And this is something that is very exciting; the ability to block infections and the whole chain of transmission.”
Without giving details, Topol said he expects to see some news from health officials about nasal spray availability in the weeks ahead.
That was December 20, 2022. So the “weeks ahead” have come and gone. What’s the matter: Biden not “thinking” about them? Maybe nasal vaccines would impede his policy of mass infection? We can’t take that chance!
NOTES
[1] From Immunity, “Sterilizing immunity: Understanding COVID-19“: “If the pathogen is eliminated before it can replicate, natural and vaccine-induced immune memory can prevent the establishment of the infection, mediating sterilizing immunity. Sterilizing immunity protects the individual and prevents transmission to new hosts, thereby contributing to protection at a population level.”
[2] Much has been made of Gillette’s AstraZenaca’s poor results with repurposing their intramuscular vaccine for nasal use. From JAMA:
Simply updating the existing vaccine constructs with new variant sequences or even making trivalent or quadrivalent vaccines covering several variants is not likely to provide the depth and breadth of protection needed to interrupt viral transmission during a prolonged period. It is also not at all clear from well-controlled clinical trials that administering existing vaccines by the intranasal route (as some countries have already even approved) will provide truly meaningful benefit over the existing generation of COVID-19 vaccines. Such limitations were recently illustrated by the disappointing results with a viral-vectored vaccine administered intranasally in an early-phase clinical trial.
See above on administration.


So, SARS-COV-2 as we’ve seen is able to get into these cells. Why can’t our delivery system just do that same thing?
Topol blocked somebody for expressing a concern which delayed my Novavax boost of mRNA-1273; until it was apparent that CDC was still ignoring several recent variants’ upticks (XBB.1.5 tsunami) through the midterms in NYC & whatever we’d likely set off in China, during the holidays?
https://mobile.twitter.com/TactNowInfo/status/1615411336015671297
Novavax is not mRNA vaccine, it’s a Spike protein vaccine, so the response is very different. Novavax has a stronger antibody but weaker t-cell response than mRNA vaccines, so I am not sure if the same concerns would apply to it.
I have two problems with this argumentation. Firstly, if the nose spray can defeat the covid virus then it can certainly defeat the flu and common cold, so fantastic…..but, hang on, if it is true and it is so obvious then why don’t we have it already?
Secondly this statement. “Although current licenced vaccines may be effective against severe disease and death…” yes, MAY be effective, because as we know there were no clinical trials done on this. The stuff was soooo great that the clinical trials were stopped and the control group injected. Way to go science.
We do know however that the mRNA leaks into all parts of the body where it produces spikes which gather on the surface of cells and trigger an immune response which can be rather large. So, why don’t we stop pushing for new treatments and start trying to fix the problems caused by the old ones?
tindrum – The problem with developing vaccines (nasal or otherwise) against coronaviruses in general, as well as adenoviruses and flu viruses, is that they mutate too fast for the vaccine developers to make new ones against the mutated viruses in time to be useful. As the viruses mutate they become better at immune evasion and replication and transmission efficiency which we see with COVID variants right now.
This is a long-standing problem. It’s why each year’s flu vaccine is actually an educated guess about which strains will be dominant six months later. (That’s how long it takes to incubate enough vaccines for public use.)
The “science” ignores an ancient method of nasal irrigation: jala neti. I didn’t bother to read all the articles (Google “jala neti prevents COVID”), but there are quite a few. Some tout iodine. One excerpt: “By giving extra hydration to your sinuses, it makes them function better. If you have a contaminant, the more you flush it out, the better you are able to get rid of dirt, viruses and anything else,” says Baxter.
“We found an 8.5-fold reduction in hospitalizations and no fatalities compared to our controls,” says senior author Dr. Richard Schwartz, chair of the MCG Department of Emergency Medicine. “Both of those are pretty significant endpoints.”
In any case, as a recent COVID sufferer who was very careful–surgical not N95 masks everywhere–I’ve begun nightly jala neti. It’s easy. One tip: the saline solution profits from the addition of baking soda. It’s less irritating with the mixture of salt and banking soda. That mixture is what the commercial neti kits offer, too.
The local testing says we’re nearing the CDC optimum of 5 cases per 100,000 tests, but doesn’t indicate whether the testing is catching all the variants. So…I rinse nightly.
I’ll keep you posted about how this works. It’s certainly less painful and inconvenient than shot after shot (I’ve had four). Oh yes, and I got an Airgami N95 mask–expensive, but worth it. No more surgical masks for me!
JFYI, the COVID I got was a bad cold with a fever. No reduction in smell or taste, but not something I’d want to experience again.
Unfortunately, the concrete remedies, like neti pots and various sprays, got left on the cutting room floor, since the post was already too long. I’ll write that material up later this week.
Meanwhile, I’m happy to have science — which doesn’t deserve your absurd shudder quotes — tell me why a neti pot might actually work; I prefer to have a mechanism, as opposed to rumor or magical thinking. Of course, your mileage may vary.
I’ve been using a mouthwash and toothpaste with chlorine dioxide for years. All good. I usually stock up when it’s on sale.
It might be worthwile to note that the listerine in mouthwash kills the bad bacteria/viruses and the good ones. There’s more and more research that shows listerine is bad for your gut health. A healthy gut is a component of the immunes system, so I fear the longterm use of mouthwash. I’ll use it (or PI) when Ive been in a risky situation like a wedding, but its not something I use every night
Might note IGM biosciences January Investor Deck pages 32-34 re the use of an ACE IgM antibody under preclinical development re Covid. I think this is different than what was previously described for them. I do not know if this approach would provoke an immune response or simply block the virus. Interesting science none the less.
Thanks for this! #Bookmarked (trying to organize my infos better!)
Things that make you go….Hmmmm
One of the many factoids about Covid that didn’t get much play/ was suppressed was in early data from Lombardy. The paper was published in NEJM, I think. This was really the first , essentially descriptive, paper telling us who got sick ( elderly, obese, HTN etc)and who didn’t ( young) based on relative risk. One nugget that didn’t get much play ( except in France, where it created a run on Nicorette), was that smokers were counterintuitively ( it is a respiratory virus, no!) protected, but not smokers who already had developed COPD.
Now one thing, smoking does, pretty much immediately, is seriously screw up mucociliary transport.
“SARS-CoV-2 progeny attach to airway microvilli 24 h post-infection and trigger formation of apically extended and highly branched microvilli that organize viral egress from the microvilli back into the mucus layer, supporting a model of virus dispersion throughout airway tissue via mucociliary transport.”
At the time – for obvious reasons – the connection was played down.
One wonders if in some alternate reality ….some curious minds had followed their nose, would we have understood this earlier ? would it have made a difference ? …….
maybe not
It’s an anecdote, but I’ve been in Japan for the 3 years since the pandemic began. Masks (surgical, not N95, but I think if everyone is wearing a mask the effect is to reduce transmission to others rather than protection of the wearer) in all public indoor spaces plus 100% remote working meant that I hadn’t nary a cold for the whole time.
A first for me, pre-pandemic my wife was always amazed and exasperated at my ability to pick up any cold going around.
Anyway I returned to my home country, Ireland, for two and half weeks for the Christmas/New Year just gone. As with the rest of the West, absolutely no masks. It was actually a bit of a culture shock to see people coughing without masks, I felt like shouting at them “FFS. Wear a mask, stop spreading your germs”.
And being too much of a coward to buck the trend, and face weird looks from family and friends, I went maskless also, though I did spray Enovid into my nose 3 times daily. But that wasn’t enough it seems, I came down with a fever for a day combined with coughing and nasal congestion (the usual pattern for my colds).
I did test negative for Covid, but wonder if the Enovid was interfering with the test.
In the end, I was fine after two days apart from the cough lingering a bit longer than usual.
Anyway, that’s my story, just to illustrate that the nasal prophylactic isn’t enough and that as Lambert often emphasizes, the Swiss cheese model of multiple imperfect protections in combination is probably the best way to go about dealing with the pandemic.
Thank you for the Enovid anecdote. I was thinking of spending the money on it, but so far I’m having good luck with Xlear (knock on wood), which is much cheaper. However I also wear an N95 and take a claritin when I go out (not medical advice). I hope you have no long term problems from your infection.
Are people really still worried about Covid?
Jawb one is don’t get it, jawb two is if you fail at jawb one don’t pass it on.
covid = airborne pathogen
Are people still worried about heart disease and all forms of cancer? Covid kills almost as many Americans, possibly more as each of these. Haven’t I heard my whole life how horrible those two types of disease are and how we should be vigilant and try to prevent them? If I could mostly prevent heart disease or cancer with a vaccine or daily nasal spray, wouldn’t I jump at the chance?
Do you know something we don’t?
What, me worry? Worry changes EVERYTHING!!!
Pre-covid life is gone. We have entered a new era. People are all unique, peoples reactions to covid the physical ailment and covid the phenomenon are also all unique. This is a long discussion topic.
Brings to mind a link from a couple days ago (1.24.2023):
Hikikomori, the Japanese phenomenon of extreme social isolation is going global ZMEScience
It’s exhausting. Disheartening. I know of five recent covid contractions in MA, OR, MT- just in my circle of good people.
Funny thing— covid could have been (and may prove to be yet- lets time capsule that and revisit in 20 years, if any of us are still ‘here’)covid could have been the catalyst for change from a ‘me first’ human behavior to ‘we first’. I am holding my breath. And wearing a KN95.
KN95— the Burka of The Woke, subject of great ire and derision in Bumphuc Flyover. Why, it’s almost like being a person with a lot of melanin in my skin?! People cross the street when I approach!
Becoming The Other. First steps toward compassion..
The only constant is change, and as for me, my mind has had it up to here… Mental Health Futures
I’m afraid that these days, people think that we who are wearing masks are sick, hence they cross the street to avoid us.
If you’re sick, buddy, don’t slap a mask on it, stay home! That’s what I would do.
I’d be happy to have people cross the street to avoid me due to my N95. Win win!!!! But it doesn’t happen here in Silicon valley.
There are so many pro-covid / antivax / antimask trolls on Twitter that come out of the woodwork to comment on any tweet that talks about covid in anything but dismissive terms, that I have to wonder if they are funded by some group or foreign government. It seems like too easy an opportunity to pass up, to weaken the US from within by weaponizing our citizens’ own stupidity. However, since China has abandoned zero covid, it seems that all governments are following the same playbook and covid is being downplayed everywhere, so that wouldn’t make a lot of sense.
I know that the US has its own crop of homegrown cranks, so foreign interference really isn’t necessary, but the sheer number of them is surprising. So, I guess it is not surprising that they would end up on Naked Capitalism, as well. What do they get out of it? Is the cognitive dissonance of covid being “over” but still seeing it discussed seriously anywhere too much for them?
For every million cranks, there must be a few thousand agents under crank cover. If the “Inner Government” wants to keep covid spreading, then the “Inner Government” would certainly seed all the troll groups and social media sites with agents to keep up the drumbeat of covid denialism, and to reinforce it if they spot it beginning to weaken.
I see no need to invoke foreign governments here.
I am. It is the elevated excess mortality rate in Britain (about 30 percent above normal) that gets my attention. I think covid is the ultimate cause.
Actually I am not sure that I am worried. I am just in the habit of avoiding fatal or debilitating disease if it is reasonably possible.
as always, NC comes through, with updates I was just wishing for. You all are amazing….. Anecdotal, have some friends here in SF and out east that got probably the new strain…and they said they’d never been so sick in their life. And pre nasal, did ‘we’ ever test those Cuban vaccines here? they might be lying, gov’ts do that, but we couldn’t even try them out?…
I look forward to future article on nasal disinfectant or prophylactic sprays other than vaccines.
Here is an interesting one I’ve discovered in Mexico.
Esteriflu disinfectant nasal spray (sorry, I couldn’t find an English version)
Google Translate of the mechanism of action description on the website:
>>Mechanism of action: ESTERIFLU® NASAL ANTISEPTIC contains active kinds of chlorine and oxygen as an active ingredient, as well as its high potential REDOX (ORP). It inactivates viruses on contact by breakage of links and denaturalisation of structural components of casings and capsids, avoiding its entrance to the host cell, preventing infection. In contact with bacteria, pollutants and bacteria, it induces oxidant damage to the depredation of electrons from its external structures, causing rupture of chemical links, extravasation of the intracellular container and osmotic lysis, destabilizing imbalance in the vital processes of the microorganism and its inactivation. Additionally, the damage caused on the surface of the pathogen can allow the entry of active species of chlorine and oxygen, which oxidize internal structures and substrates, assisting in their elimination.
>>The concentration of active kinds of chlorine and oxygen and the neutral pH of ESTERIFLU® NASAL ANTISEPTICO ensure controlled biocidal activity, being harmless to human anatomy.
Relevant small open-label study showing efficacy against Covid, almost two years old, summary in English: Oropharyngeal sanitization with electrolyzed superoxidation solution with neutral pH to prevent COVID-19
Other sprays that have already been discussed by Lambert in the past:
Sanotize (brand names: Enovid, Virx, Fabispray, in different countries)
Carageenan-based nasal sprays (Betadine)
Povidone iodine + saline solutions
Using Xylitol, saline, grapefruit seed enzyme spray for (excellent, conscientious MIRV13/ UVC HVAC) dentist on Friday. I’d used Cromalyn Sodium/ Nicotinamide riboside/ B12/ RG3 spray & peroxide sprays after long mass transit rides? Have yet to try NO precursor nose sprays (has anybody, here?)
Enovid/sanotize is a NO spray. (I don’t understand the “precursor” bit.) My wife and I use it with regular N95 use and so far, so good, save for one respiratory episode down to unguarded time with well-disciplined grandchildren that tested Covid-negative all around. Like EarlyGray above, I wonder if Enovid compromised our testing…
Really, it’s just being POOR. Both the NONS & Synapsin ideas predate SARS CoV2 & Betadine, Xylitol or peroxide sprays predate plastic sprayers. A year back, I’d got my 2nd (BA.2) during a root canal (N95 on both, HEPA filter running full tilt, but most of the YOUNG staff, got it & none was sure if it was their kids or proximity to open bathroom door?) I’d been using precursors L-citrulline, L-arginine, beets & maritime pine bark I’d used for ED for the first time @ 68yrs of age, from PASC (Nattokinase, NAC & Serrapeptase seem to work better & you can sorta make your own NO with 4, 7, 8 breathing, believe it or not?)
Husband and I also use Enovid and so far so good, I’ve put a lot of faith in it. The drawback is the cost $35-$40 per bottle though.
Nicotinoids! The devil in the flower seed coating. How simply, elegantly, clever?!
I wonder why we are chasing complicated genetic mRNA versus the freely available ubiquitous alternatives that have proven efficacy- Oregano is a known anti-bacterial. Nicotine… we, we all know about that !
Hmmmm, must have something to do with complexity, ownership, and profits, preying on fear relating to the the ultimate personal concern: the health of one’s loved ones, and self.
THAT’s the business to be in! Imagine if we turned health care into a Utility?!
FWIW:
https://www.drlamcoaching.com/blog/synapsin-brain-fog-fatigue-and-more/
We’d gotten it SO quickly in Mar of ’20, I’d previously used zinc, D3, C & Quercitin (ancient Kraut secret for coronavirus) in swab form, while working 84hr (91hr) weeks, on the road in SCARY mills. 3 friends >70yrs had D614.G while working. As far as I know, none has died of stroke or MI, yet? We’d such a mild case. We’d been shocked, when blood oxygen dropped <89% on day 15? We could still hold our breath, no fever, little congestion? Wonder what happened to the lettuce protein chewing gum, University of Pennsylvania made as prophylaxis for HCW & school kids.
It would be good to take a claritin, too, before you go, and even another one that evening. That is, if you have no medical reasons to avoid taking claritin.
Dogs have nasal vaccines. It’s standard for Kennel Cough. Cats have them, too.