By Rajiv Sethi, Professor of Economics at Barnard College, Columbia University. Originally published at his website
In my last post I looked at Sweden’s pandemic response and made two observations.
First, it appears that Sweden’s policy choices during the pandemic, which relied largely on voluntary compliance with public health guidance rather than mandates, do not seem to have resulted in superior economic performance relative to its Nordic neighbors. Economic growth in Norway, Denmark, and Sweden followed very similar trajectories over the 2020-2022 period.
Second, there were significant differences across these countries in excess death rates early in the pandemic, with more loss of life in Sweden, but cumulative excess death rates appear to have converged. That is, the Swedish polices affected the timing rather than eventual magnitude of excess mortality. Denmark and Norway were able to postpone excess deaths (relative to Sweden) but not avoid them entirely.
How can these two observations be reconciled? One can explain the economic trajectories by arguing that Swedes voluntarily did what their neighbors were pressured or compelled to do. But this would not explain the pattern of excess deaths. It appears that the main difference between Sweden and its neighbors was the degree to which the most vulnerable populations (the elderly and those with weakened immune systems or serious heart and lung conditions) were protected. The state epidemiologist Anders Tegnell recognized this, while defending Sweden’s overall strategy of reliance on personal responsibility and voluntary compliance.
But there were many other factors at play, including very high vaccination rates in Sweden (perhaps in the shadow of the trauma caused by early excess mortality). Following my earlier post I got a long and thoughtful message from Troy Tassier of Fordham University which discusses some of these issues. I have reproduced his message below with permission.
Hi Rajiv,
I hope that you are doing well. I read your blog post on Sweden with interest today. I have been interested in the “catch-up” in excess deaths by the non-Sweden Nordic countries for a while. It’s very perplexing to me and I haven’t done a really deep dive but I had a few comments that may be of interest to you.
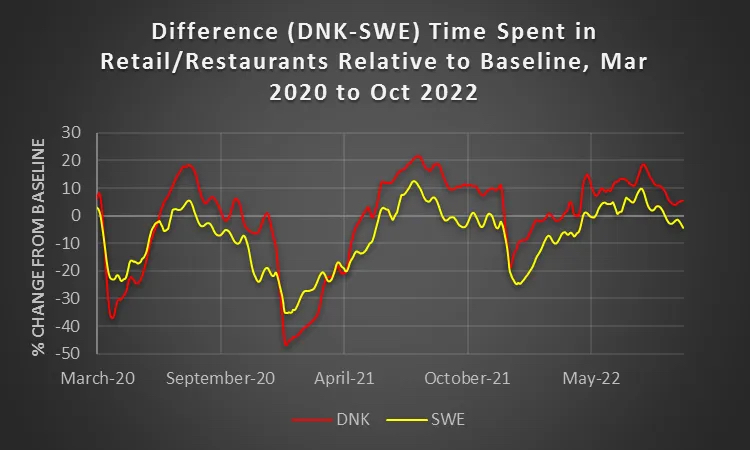
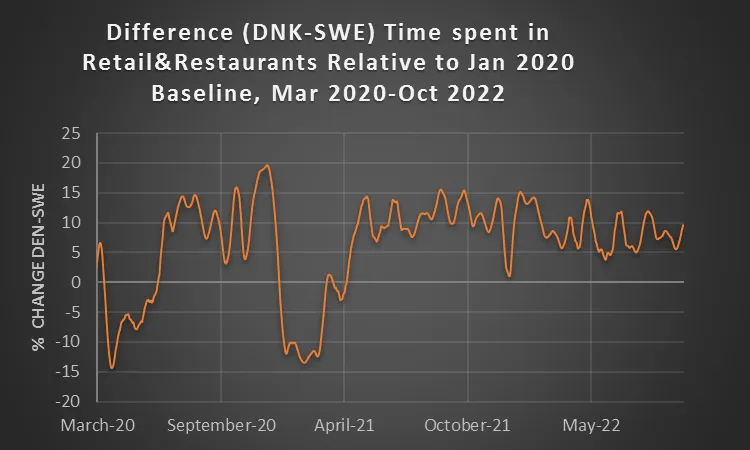
It seems that there is a difference between what I’ll call the “folklore” of Swedish policy and the reaction of Swedish residents. If you look at various mobility metrics (like Google’s mobility data) it appears that the Swedish population didn’t behave all that differently than populations of neighboring countries despite Sweden being less aggressive in terms of its official policy response. Note the two graphs below which are based on Google data gathered from OWiD, smoothed to a weekly average. (Comparisons to other Nordic countries and comparisons using other Google metrics like Time Spent at Home are similar.) Other than the initial pandemic phase in spring 2020 and the winter of 20/21 the Swedish population actually had more conservative behavior than Denmark. They cut back on mobility more than Denmark except for those two periods of time. Because the Swedish population didn’t respond strongly in spring 2020 I think this goes a long way in explaining why Sweden did so poorly in terms of excess deaths. And, it may explain a part of the catch-up by other Nordics (because the Swedish population was actually more careful than the other Nordic populations in 22/23). But I don’t think it can explain all of it. I think it is also interesting that after Sweden did so poorly in 2020 that the population reacted more strongly in future months. Part of me wonders if there was a NYC type effect where things were so bad that people acted strongly in order to avoid a repeat of 2020. So they locked themselves down because of their risk perception from previous experience.
I think point 1 also gives clues as to why Sweden’s economic performance wasn’t appreciably better than its neighbors. The Swedish population didn’t behave all that differently than its neighbors so its economy suffered and then rebounded to a similar degree.
The mobility point above also suggests what I’ll call strong agency effects of populations. Not surprisingly the mapping from policy to behavior isn’t direct. And, like the Sweden graph below, there is evidence that people act to avoid (pandemic) risk without being told to do so—no surprise to an economist that people respond to perceived risk, right?! For instance, Austan Goolsbee and Chad Syverson suggest that only a small percent of the decrease in economic behavior was due to policy choices/ laws early in the pandemic. And similar to that paper, if you look to things like Google data on time in public transit stations, time spent at home, etc., the majority of the response in March 2020 occurred prior to specific “stay at home” announcements or schools closures. I have a small bit on this concerning NYC and London in a book I have coming out this February. So again, Sweden’s official policies (or lack of policy response) doesn’t mean that Sweden’s population didn’t react. They did and over a large part of the pandemic they responded more strongly than their neighbors despite no policy telling or suggesting that they do so.
All of this still doesn’t explain why the Nordics ended up in the same place as Sweden in terms of excess deaths after 3+ years. I have seen a couple of possibilities suggested (other than the obvious—it was going to happen no matter what policy choice was made and the public health measures implemented in 2020 just delayed the inevitable):
I don’t have a good cite off hand for this but I have been part of conversations suggesting that Sweden did a much better job at getting vaccines to its elderly and most vulnerable populations. And they did this more quickly than their neighbors. This suggests that the catch-up in excess deaths may have been because Sweden’s vaccine policy was more responsive than their neighbors. Which again is a different story than the one that dominates public perception (i.e., that Sweden did nothing). Sweden may have done well simply because they had a really aggressive and swift vaccine policy.
I don’t know enough about this, but I am somewhat skeptical of the way that many excess death calculations are estimated. Many don’t seem to account for changes in populations. Some are simple linear regressions of short term trends, like 3-5 years, sometimes adjusting for age composition and sometimes not. Almost none take account of demographic factors like migration and changing demographics. I’d love to see a paper that really pulls apart how these estimates are made. My quick reading of public health commentary on this suggests that there are initially unintuitive effects of things like immigration. For instance even though recent immigrants tend to be poorer on average, they tend to be healthier (otherwise they couldn’t migrate). Then there are replacement effects during pandemics—if vulnerable members of a population die early in a pandemic then expected deaths in future years should decrease because people who you may expect to die in year three from some “natural cause” die in year one due to an epidemic—so your expected deaths should be lower in year three than initial estimates suggest. But a linear estimate of pre-pandemic years is going to miss this. There will be a sort of natural mean reversion if you don’t account for the underlying change in the population as the epidemic evolves. So, there seem to be a host of factors that are not accounted for by a number of the excess death estimates that I have seen. Maybe these are all small magnitude effects that don’t really matter. But Sweden v. other Nordics in late 2021 and 2022 really puzzle me. In the end it may simply be that there was nothing we could do except delay the inevitable. The optimist in me hopes this isn’t true. But I’d love to understand this better.
Anyway, no real reason or action plan for sending this to you. Just wanted to throw out some unorganized thoughts that I had after reading your post a bit earlier today.
Best,
Troy
Troy has a Substack newsletter in case you’d like to subscribe.
One final thought. The focus on Sweden’s approach is understandable, since it was such an outlier and received a great deal of contempt and scorn at the time. But the data suggests that one ought also to look closely at the policies instituted in Norway and (especially) Denmark. On both economic and public health grounds Denmark appears to have done extremely well relative to its neighbors, though at the cost of some liberties that Swedes continued to enjoy.
I am often left with the discrepancy between the apparent lack of serious and potent effort to collect, manage and report on verifiable and consistent data and how frightful and horrific the “pandemic” really is.
If it was to terrible, and was such a risk to all, wouldn’t the effort be greater?
CanCyn
Depends on whose risk and what kind of risk you’re talking about. The health of us mere citizens? Not so important. The economy, or at least the part of that works for big pharma, big corporations and shareholders? The latter is very important to those people and so, you get little in the way of « serious and potent effort to collect, manage and report on verifiable and consistent data«
DJG, Reality Czar
Yep, I am already seeing YouTube videos from people like Robbie Soave at Rising and Jimmy Dore (of Big Blind Spot about Covid and Its Significance) ballyhooing the Swedish figures.
Quoting Troy Tessier from above: “So again, Sweden’s official policies (or lack of policy response) doesn’t mean that Sweden’s population didn’t react. They did and over a large part of the pandemic they responded more strongly than their neighbors despite no policy telling or suggesting that they do so.”
There is no reason whatsoever to apply the Swedish experience to the U S of A. Let me repeat that: There is no reason whatsoever to apply the Swedish experience to the U S of A, which what is likely to come of these analyses.
Why? The self-destructive individualism of Americans truly doesn’t have a counterpart in Scandinavia, even in Sweden. The long centuries of a rather Pietist Lutheranism in these countries, plus years of social-democratic politics, mean that the members of the public there are much more aware of the needs of their fellow citizens. They also are smaller, less populated countries, where, in a real sense, everyone knowns everyone.
To wit: Just how many push-and-shoving matches outside a Red Lobster or inside a grocery store were posted from Scandinavia?
So: The results are “interesting,” and they apply only to Scandinavia. Basing any U.S. policy on them is impossible. Did I type impossible? Yes, I did.
SteveD
I like the “Big Blind Spot about Covid” framing of Dore, however I would suggest it is not purely blind: His livelihood depends on the public feeling safe and free to gather in clubs and pay for his standup shows. That aside, I cringe whenever he launches into another “it’s just like a cold; get over it” rant.
truly
And to be fair, he was/is vaccine injured. Nothing like being injured by a medicine that is forced upon the public to open your eyes up a bit.
Jeff
His career is mostly online.
digi_owl
Sadly, thanks media being addicted to USA, we are adopting US behaviors and attitudes.
Basil Pesto
The author makes an error in assuming that Sweden’s near neighbours (relevant points of comparison, btw, but not the only ones) and indeed the world entire didn’t shift their policy at all for two years when of course they did: they switched in 2021 to a vaccine-rationalised version of Sweden’s policy. In that context it’s inevitable that they converged, but one doesn’t have to be especially utopian, I don’t think, to understand that there was a policy alternative to the state of failure that the world now finds itself in, and which Sweden along with the US and UK, pioneered* before the rest of the world joined them, using vaccines to rationalise that policy change. As I’ve been saying for a while, we’re all Sweden now.
Thus it’s no surprise that these countries converged. Sweden let rip in year one with individuals left to fend for themselves and burnt off much of its ‘dry tinder’ (Tegnell’s own wording, by which he meant the elderly and clinically vulnerable). The other countries did this in 2021, with the addition of vaccines (which clearly made a positive difference, but a difference which in the long run will prove to be transient and insufficient for optimal outcomes (which, let’s say for the sake of argument, are a return to the homeostatic state of the impact of preventable infectious diseases in the developed world in 2019), and which will in turn result in more dry tinder burn-off and considerable immiseration and ill health besides.
To wit (and unsurprisingly), the author ignores the long tail of Infinite Maximum SARS because of course he does. Here’s one article to which he can turn. Again, this statement will be an obvious truism to most (?) NC commenters, but the anecdata in that link (which complements actual data) describes a big problem which is only going to get worse.
* The US and UK had restrictions, yes, but of the ultimately inadequate and protracted ‘Flatten the Curve’ kind which were not up to solving the problem, and which Swedes to an extent seemed to impose upon themselves (which, naturally, resulted in less favourable outcomes in 2020 than the state-enforced version) per the author of this piece. It’s comparing a shit sandwich to a shit stew. Compare this with, say, Australia and New Zealand – to name just two – whose sub-jurisdictions solved the problem several times and whose people enjoyed, for those periods, real ~Freedom~ evinced not just by, say, my ability in December 2020 to go to bars, restaurants, gigs, travel interstate to spend Christmas with my family, all that nice stuff, but also with no threat of catching and transmitting a transparently harmful disease, a state of freedom which nobody on the planet enjoys any longer, reversing the incredible gains in public heath made in the 20th century in the name of the maximally unimpeded welfare of capital markets over people, and powered by some truly unhinged and murderous libertarian (or pseudo-libertarian, if you prefer) ideology. By contrast, at the same time, winter 2020 in NYC, morgue trucks were being fired up and huge segments of not just the elderly but that city’s working population were being killed off because those inadequate half-measure restrictions were not up to the task. But Australia and NZ will now converge with Europe too, because they have adapted their policy. And if turns out that we are in what later may in retrospect end up being thought of as an “omicron holiday”, then all bets are off.
(sorry if this reads poorly or confusingly, writing the post on my phone)
Adam1
I agree. The lock downs were meant to attempt to do 2 things… A) TRY & stop covid entirely; B) slow its spread enough to keep the healthcare systems from collapsing.
For the most part the west was spared healthcare collapse and now that we’ve given up on irradiating covid it seems only logical that deaths would trend towards convergence.
COUNT MARCO
There was no real danger of “healthcare collapse” except the initial (and in PART, understandable lack of clarity about incident fatality rates…i.e., when ‘officials’ were PROJECTING an IFR of over 3%.. which was later quantitively shown to be a tiny fraction of that.
All of us who are presumably intelligent readers should know all of this by now. This correction of the original doomsaying was originally published by John Ioannidis, et al by Aug 25 2020… that’s 2020, see at / and replicated many many times since then.
The Collapse Scenario evaporated when the hospital ships were quietly sent home and tent cities in NYC parks abandoned and sent packing.
Why can we not all start to agree on a basic set of facts-on-ground WITHOUT RANCOR???
Skip Intro
This is a great point. We’re all Sweden now.
As Sweden’s better focus and effectiveness in delivering vaccines to the most vulnerable was floated as a reason why their worse policies didn’t lead to worse results in all-cause mortality, I recalled a study that showed the mRNA vaccines did not, themselves, reduce mortality, but seemingly shifted it from Covid. So in terms of mortality, vaccination levels should be neutral, though they can move the deaths out of the covid column.
DJG, Reality Czar
Basil Pesto: Many thanks for your comment and your insights. I have one quibble (and note that above I use the phrase “self-destructive individualism”):
unhinged and murderous libertarian (or pseudo-libertarian, if you prefer) ideology
By on their meretricious face, libertarian ideas are murderous and self-destructive. Libertarians want to sacrifice people to money and to their fantasies of personal (transactional) relationships. So let’s call a spade a spade, a shovel a shovel, a casual murderer a casual murder.
some guy
It has been said that “breathing is a social relation”. But that is only true for pro-social people.
When anti-social people ( Typhoid Mary covid zombies, ” muh No Mask freeduhm” droids, etc.) practice breathing, they practice breathing as an act of anti-social aggression.
I bring this up because at some point in the past, somebody noted that wearing a mask with an air-outlet exhaust valve was not protecting others, but only protecting oneself; hence not as pro-social as a no-outlet mask would be. But when pro-social people are surrounded by anti-social pro-disease people, there is no point in trying to protect the anti-protection people. Best to focus on protecting oneself first, and then protecting the protection-capable by getting them to wear masks too. And if an exhaust outlet makes a mask more individual user friendly and hence makes itself more likely to be worn, better that than maskless.
” Look for the helpers” makes good sense as the helpers try to grow a growing community of co-helpers. It also makes sense to look for the hurters in order to avoid them. And to avoid helping them because helping a hurter only helps a hurter to hurt others more effectively. Which is what the hurter lives to do.
GM
Note that Sweden let it rip, but despite that people didn’t actually get infected in huge numbers.
Which seems to be because of a combination of Swedes being socially distant by default and some real measures nevertheless still being taken.
I recall they did a serosurvey in summer of 2020 in Stockholm and the attack rate was well below 10%. It looks like it didn’t reach much above 30% before vaccination started. Then vaccination reached high coverage, and on top of it all, Sweden does have very good hospitals (even if it actively denied care to many elderly people), and this is why overall mortality is so low, despite the openly genocidal policies adopted.
Which is good for the 70-80,000 Swedes that didn’t die but would have died with the same policies and the same contacts rates and shitty healthcare as in South America or Eastern Europe.
But very bad for the world because it seems like it “validated” the Swedish approach.
Roland
We all converged on the same basic blunders. Tegnell was just bolder than the rest–and surrendered first.
OTOH, if the whole world had copied PRC, the crisis probably would have ended within a few months.
Instead, we all lost the war, our world is now under enemy occupation, and we have to hope that our conqueror will not impose too heavy a tribute in the years to come.
Futility
“OTOH, if the whole world had copied PRC, the crisis probably would have ended within a few months.”
One is not allowed to say this. The recent abandonment of strict Covid measures in China now “proves” that this approach was doomed right from the start when in fact it only shows the inability of the rest of the world (with the exemption of New Zealand, Australia) to follow through. The fact that after an imposed lock-down the number of cases plummeted precipitously is also irrelevant since now even cats or moose carry the virus.
TimH
Don’t forget “Evaluation of science advice during the COVID-19 pandemic in Sweden”
The Swedish people were kept in ignorance of basic facts such as the airborne SARS-CoV-2 transmission, that asymptomatic individuals can be contagious and that face masks protect both the carrier and others. Mandatory legislation was seldom used; recommendations relying upon personal responsibility and without any sanctions were the norm. Many elderly people were administered morphine instead of oxygen despite available supplies, effectively ending their lives.
maipenrai
Sweden is older than Norway. Sweden has more immigrants from non European countries than Norway.
curlydan
I ran across this (translated) Swedish “chat” that asked people about their long-term Covid symptoms. After getting tons of comments, they cut the chat off. The stories are heartbreaking.
They euthanized their elderly (over 65?) , or were accused by relatives of doing so, by withholding oxygen from those suffering from hypoxia, and giving them opium instead, which eases the symptoms but not the cause.
TimH
Opiates depress respiration. It’s a good way to kill those with hypoxia… so a lot more than ‘eases the symptoms’.
Terry Flynn
Opiates depress respiration. It’s a good way to kill those with hypoxia
Indeed. I quickly advised family to quit using cocodamol when the pandemic struck.
On the subject of Swedish “norms” I remember a meme re Sweden at the time saying something like “this social distancing rule is awful. I don’t want to get closer to other people!” For those of us who’ve lived there, it’s funny because it’s true. When I was having maximum problems integrating in Uppsala, a Swedish professor (originally from Stockholm) took me out for coffee and cake and explained that 15+ years there *still* wasn’t enough to be considered an “insider”. Thus, it genuinely “wasn’t me”.
On a lighter but cynical note, how to turn John Carpenter’s cult classic “The Thing” into the most boring movie ever. Set it in Sweden. The monster dies in act one of loneliness and malnutrition. /s
Harold
Well, yes. That’s why it’s given to dying patients.


I am often left with the discrepancy between the apparent lack of serious and potent effort to collect, manage and report on verifiable and consistent data and how frightful and horrific the “pandemic” really is.
If it was to terrible, and was such a risk to all, wouldn’t the effort be greater?
Depends on whose risk and what kind of risk you’re talking about. The health of us mere citizens? Not so important. The economy, or at least the part of that works for big pharma, big corporations and shareholders? The latter is very important to those people and so, you get little in the way of « serious and potent effort to collect, manage and report on verifiable and consistent data«
Yep, I am already seeing YouTube videos from people like Robbie Soave at Rising and Jimmy Dore (of Big Blind Spot about Covid and Its Significance) ballyhooing the Swedish figures.
Quoting Troy Tessier from above: “So again, Sweden’s official policies (or lack of policy response) doesn’t mean that Sweden’s population didn’t react. They did and over a large part of the pandemic they responded more strongly than their neighbors despite no policy telling or suggesting that they do so.”
There is no reason whatsoever to apply the Swedish experience to the U S of A. Let me repeat that: There is no reason whatsoever to apply the Swedish experience to the U S of A, which what is likely to come of these analyses.
Why? The self-destructive individualism of Americans truly doesn’t have a counterpart in Scandinavia, even in Sweden. The long centuries of a rather Pietist Lutheranism in these countries, plus years of social-democratic politics, mean that the members of the public there are much more aware of the needs of their fellow citizens. They also are smaller, less populated countries, where, in a real sense, everyone knowns everyone.
To wit: Just how many push-and-shoving matches outside a Red Lobster or inside a grocery store were posted from Scandinavia?
So: The results are “interesting,” and they apply only to Scandinavia. Basing any U.S. policy on them is impossible. Did I type impossible? Yes, I did.
I like the “Big Blind Spot about Covid” framing of Dore, however I would suggest it is not purely blind: His livelihood depends on the public feeling safe and free to gather in clubs and pay for his standup shows. That aside, I cringe whenever he launches into another “it’s just like a cold; get over it” rant.
And to be fair, he was/is vaccine injured. Nothing like being injured by a medicine that is forced upon the public to open your eyes up a bit.
His career is mostly online.
Sadly, thanks media being addicted to USA, we are adopting US behaviors and attitudes.
The author makes an error in assuming that Sweden’s near neighbours (relevant points of comparison, btw, but not the only ones) and indeed the world entire didn’t shift their policy at all for two years when of course they did: they switched in 2021 to a vaccine-rationalised version of Sweden’s policy. In that context it’s inevitable that they converged, but one doesn’t have to be especially utopian, I don’t think, to understand that there was a policy alternative to the state of failure that the world now finds itself in, and which Sweden along with the US and UK, pioneered* before the rest of the world joined them, using vaccines to rationalise that policy change. As I’ve been saying for a while, we’re all Sweden now.
Thus it’s no surprise that these countries converged. Sweden let rip in year one with individuals left to fend for themselves and burnt off much of its ‘dry tinder’ (Tegnell’s own wording, by which he meant the elderly and clinically vulnerable). The other countries did this in 2021, with the addition of vaccines (which clearly made a positive difference, but a difference which in the long run will prove to be transient and insufficient for optimal outcomes (which, let’s say for the sake of argument, are a return to the homeostatic state of the impact of preventable infectious diseases in the developed world in 2019), and which will in turn result in more dry tinder burn-off and considerable immiseration and ill health besides.
To wit (and unsurprisingly), the author ignores the long tail of Infinite Maximum SARS because of course he does. Here’s one article to which he can turn. Again, this statement will be an obvious truism to most (?) NC commenters, but the anecdata in that link (which complements actual data) describes a big problem which is only going to get worse.
* The US and UK had restrictions, yes, but of the ultimately inadequate and protracted ‘Flatten the Curve’ kind which were not up to solving the problem, and which Swedes to an extent seemed to impose upon themselves (which, naturally, resulted in less favourable outcomes in 2020 than the state-enforced version) per the author of this piece. It’s comparing a shit sandwich to a shit stew. Compare this with, say, Australia and New Zealand – to name just two – whose sub-jurisdictions solved the problem several times and whose people enjoyed, for those periods, real ~Freedom~ evinced not just by, say, my ability in December 2020 to go to bars, restaurants, gigs, travel interstate to spend Christmas with my family, all that nice stuff, but also with no threat of catching and transmitting a transparently harmful disease, a state of freedom which nobody on the planet enjoys any longer, reversing the incredible gains in public heath made in the 20th century in the name of the maximally unimpeded welfare of capital markets over people, and powered by some truly unhinged and murderous libertarian (or pseudo-libertarian, if you prefer) ideology. By contrast, at the same time, winter 2020 in NYC, morgue trucks were being fired up and huge segments of not just the elderly but that city’s working population were being killed off because those inadequate half-measure restrictions were not up to the task. But Australia and NZ will now converge with Europe too, because they have adapted their policy. And if turns out that we are in what later may in retrospect end up being thought of as an “omicron holiday”, then all bets are off.
(sorry if this reads poorly or confusingly, writing the post on my phone)
I agree. The lock downs were meant to attempt to do 2 things… A) TRY & stop covid entirely; B) slow its spread enough to keep the healthcare systems from collapsing.
For the most part the west was spared healthcare collapse and now that we’ve given up on irradiating covid it seems only logical that deaths would trend towards convergence.
There was no real danger of “healthcare collapse” except the initial (and in PART, understandable lack of clarity about incident fatality rates…i.e., when ‘officials’ were PROJECTING an IFR of over 3%.. which was later quantitively shown to be a tiny fraction of that.
All of us who are presumably intelligent readers should know all of this by now. This correction of the original doomsaying was originally published by John Ioannidis, et al by Aug 25 2020… that’s 2020, see at / and replicated many many times since then.
The Collapse Scenario evaporated when the hospital ships were quietly sent home and tent cities in NYC parks abandoned and sent packing.
Why can we not all start to agree on a basic set of facts-on-ground WITHOUT RANCOR???
This is a great point. We’re all Sweden now.
As Sweden’s better focus and effectiveness in delivering vaccines to the most vulnerable was floated as a reason why their worse policies didn’t lead to worse results in all-cause mortality, I recalled a study that showed the mRNA vaccines did not, themselves, reduce mortality, but seemingly shifted it from Covid. So in terms of mortality, vaccination levels should be neutral, though they can move the deaths out of the covid column.
Basil Pesto: Many thanks for your comment and your insights. I have one quibble (and note that above I use the phrase “self-destructive individualism”):
unhinged and murderous libertarian (or pseudo-libertarian, if you prefer) ideology
By on their meretricious face, libertarian ideas are murderous and self-destructive. Libertarians want to sacrifice people to money and to their fantasies of personal (transactional) relationships. So let’s call a spade a spade, a shovel a shovel, a casual murderer a casual murder.
It has been said that “breathing is a social relation”. But that is only true for pro-social people.
When anti-social people ( Typhoid Mary covid zombies, ” muh No Mask freeduhm” droids, etc.) practice breathing, they practice breathing as an act of anti-social aggression.
I bring this up because at some point in the past, somebody noted that wearing a mask with an air-outlet exhaust valve was not protecting others, but only protecting oneself; hence not as pro-social as a no-outlet mask would be. But when pro-social people are surrounded by anti-social pro-disease people, there is no point in trying to protect the anti-protection people. Best to focus on protecting oneself first, and then protecting the protection-capable by getting them to wear masks too. And if an exhaust outlet makes a mask more individual user friendly and hence makes itself more likely to be worn, better that than maskless.
” Look for the helpers” makes good sense as the helpers try to grow a growing community of co-helpers. It also makes sense to look for the hurters in order to avoid them. And to avoid helping them because helping a hurter only helps a hurter to hurt others more effectively. Which is what the hurter lives to do.
Note that Sweden let it rip, but despite that people didn’t actually get infected in huge numbers.
Which seems to be because of a combination of Swedes being socially distant by default and some real measures nevertheless still being taken.
I recall they did a serosurvey in summer of 2020 in Stockholm and the attack rate was well below 10%. It looks like it didn’t reach much above 30% before vaccination started. Then vaccination reached high coverage, and on top of it all, Sweden does have very good hospitals (even if it actively denied care to many elderly people), and this is why overall mortality is so low, despite the openly genocidal policies adopted.
Which is good for the 70-80,000 Swedes that didn’t die but would have died with the same policies and the same contacts rates and shitty healthcare as in South America or Eastern Europe.
But very bad for the world because it seems like it “validated” the Swedish approach.
We all converged on the same basic blunders. Tegnell was just bolder than the rest–and surrendered first.
OTOH, if the whole world had copied PRC, the crisis probably would have ended within a few months.
Instead, we all lost the war, our world is now under enemy occupation, and we have to hope that our conqueror will not impose too heavy a tribute in the years to come.
“OTOH, if the whole world had copied PRC, the crisis probably would have ended within a few months.”
One is not allowed to say this. The recent abandonment of strict Covid measures in China now “proves” that this approach was doomed right from the start when in fact it only shows the inability of the rest of the world (with the exemption of New Zealand, Australia) to follow through. The fact that after an imposed lock-down the number of cases plummeted precipitously is also irrelevant since now even cats or moose carry the virus.
Don’t forget “Evaluation of science advice during the COVID-19 pandemic in Sweden”
https://doi.org/10.1057/s41599-022-01097-5
Sweden is older than Norway. Sweden has more immigrants from non European countries than Norway.
I ran across this (translated) Swedish “chat” that asked people about their long-term Covid symptoms. After getting tons of comments, they cut the chat off. The stories are heartbreaking.
https://www-svt-se.translate.goog/nyheter/lokalt/stockholm/chatt-har-du-kvar-symtom-efter-covid?_x_tr_sl=sv&_x_tr_tl=en&_x_tr_hl=en&_x_tr_pto=sc
No one mentioned this: https://pandemicaidnetworks.org/articles/scathing-criticism-for-treatment-of-the-elderly-in-sweden
They euthanized their elderly (over 65?) , or were accused by relatives of doing so, by withholding oxygen from those suffering from hypoxia, and giving them opium instead, which eases the symptoms but not the cause.
Opiates depress respiration. It’s a good way to kill those with hypoxia… so a lot more than ‘eases the symptoms’.
Indeed. I quickly advised family to quit using cocodamol when the pandemic struck.
On the subject of Swedish “norms” I remember a meme re Sweden at the time saying something like “this social distancing rule is awful. I don’t want to get closer to other people!” For those of us who’ve lived there, it’s funny because it’s true. When I was having maximum problems integrating in Uppsala, a Swedish professor (originally from Stockholm) took me out for coffee and cake and explained that 15+ years there *still* wasn’t enough to be considered an “insider”. Thus, it genuinely “wasn’t me”.
On a lighter but cynical note, how to turn John Carpenter’s cult classic “The Thing” into the most boring movie ever. Set it in Sweden. The monster dies in act one of loneliness and malnutrition. /s
Well, yes. That’s why it’s given to dying patients.