Yves here. While the AMA did have a big role in stopping the implementation of some version of public health care, they were far from the only bad actor. It would be unfortunate if this description of the AMA’s successful tactics were to obscure the role of US labor unions. They too opposed government-provided health care. They wanted it to be a key contract bennie so as to justify the need for union negotiations and therefore union dues. Mind you, there are many ways unions help workers, as we see from unions overseas not falling over in droves abroad in Europe after those countries implemented their government-paid regimes. So the union conduct was particularly disgraceful since it benefited the leadership while not helping the rank and file and hurting broad swathes of Americans.
And while doctors are getting a comeuppance via the horrible crapification of American medicine, which is being visited upon them as well as patients, it’s not as if the current generation of doctors were part of the anti-government-medicine campaign. This is the professional version of the children paying for the sins of the fathers.
By Marcella Alsan, Angelopoulos Professor of Public Policy Harvard Kennedy School; Yousra Neberai, Graduate student in Public Policy Harvard University; and Xingyou Ye, PhD Student Princeton University. Originally published at VoxEU
The US healthcare system relies on a heavily subsidised and lightly regulated private sector, and despite living in the world’s wealthiest country, millions of Americans remain uninsured, underinsured, or unsure of their coverage. This column examines the rise of private health insurance after WWII, when the American Medical Association – an interest group representing physicians – financed a nationwide campaign against National Health Insurance. Directed by the country’s first political public relations firm, the campaign used mass advertising to associate NHI with socialism and private insurance with the ‘American Way’.
The Sustainable Development Goals (SDGs) devised by the UN have advanced the target of achieving universal health coverage (UHC) for all countries by 2030 (Eozenou et al. 2023). This goal has already been reached by most high-income countries, but a notable exception is the US. Despite living in the wealthiest country in the world, millions of Americans remain uninsured, underinsured, or unsure of their coverage (Blumenthal and Collins 2022, Scott 2023a). Medical debt continues to be the leading cause of personal bankruptcy, and US performance on several key health outcomes is consistently below that of peer nations (Schneider et al. 2021, Kluender et al. 2021, Papanicolas et al. 2018). Recently, prominent health economists have pointed to the US healthcare system, with its reliance on a heavily subsidised, lightly regulated private sector, as an integral part of the problem (Case and Deaton 2020, Einav and Finkelstein 2023).
In a recent paper (Alsan et al. 2024), we step back from this current debate and seek to understand how the US developed its anomalous healthcare system. Typical explanations include a history of individualistic culture, union bargaining, inflationary pressure, or favourable tax treatment for employer-sponsored health insurance (Scott 2023b). We investigate another potential contributing factor: a large-scale post-WWII marketing campaign funded by the interest group representing physicians – the American Medical Association (AMA) – in coordination with other industries. The campaign was managed by the world’s first political public relations firm, Whitaker and Baxter’s (WB) Campaigns Inc. Although the campaign has been discussed previously – most notably in a New Yorker profile of Whitaker and Baxter (Lepore 2012) – to our knowledge, our paper provides the first rigorous analysis of whether and to what extent the interest-group financed campaign, which relied heavily on the indirect lobbying of voters, shaped the health insurance landscape during a critical juncture.
The campaign came about quickly in response to what the AMA described as an “Armageddon moment”. The reason for the AMA’s alarm was manifold: first, events abroad – notably, the introduction of the National Health Service (NHS) in the UK – provided an example of state-sponsored healthcare from a country which shared a common language and legal tradition. Second, the shocking 1948 election of Harry Truman brought a strong backer of national health insurance into the White House alongside a commanding Democratic majority in Congress – guaranteeing the topic would be on the legislative agenda. Third, Americans were highly in favour of national insurance and a leading rationale was purportedly a concern for those less fortunate.
The AMA-WB campaign had two key components. First, they used mass advertising to associate NHI with socialism, while the private (or voluntary) insurance option was described as the “American Way”. These advertising efforts of the AMA were complemented by tie-in advertising from other industries fearing a return to war-time price controls. In addition, the strategy called on AMA doctors to discuss private health insurance with their patients and to distribute pamphlets echoing the individualistic advertising message (see Figure 1). Through local and state medical organizations, physicians looking to defray medical costs had organised their own insurance product, which came to be known as Blue Shield, and they were eager for enrolees. All told, approximately $250 million (in current terms) was spent to sway voters, an unprecedented amount for the time. Doctors were also instructed to use their prestige to urge local civic organisations to pass resolutions against national health insurance.
Figure 1 Campaign pamphlets
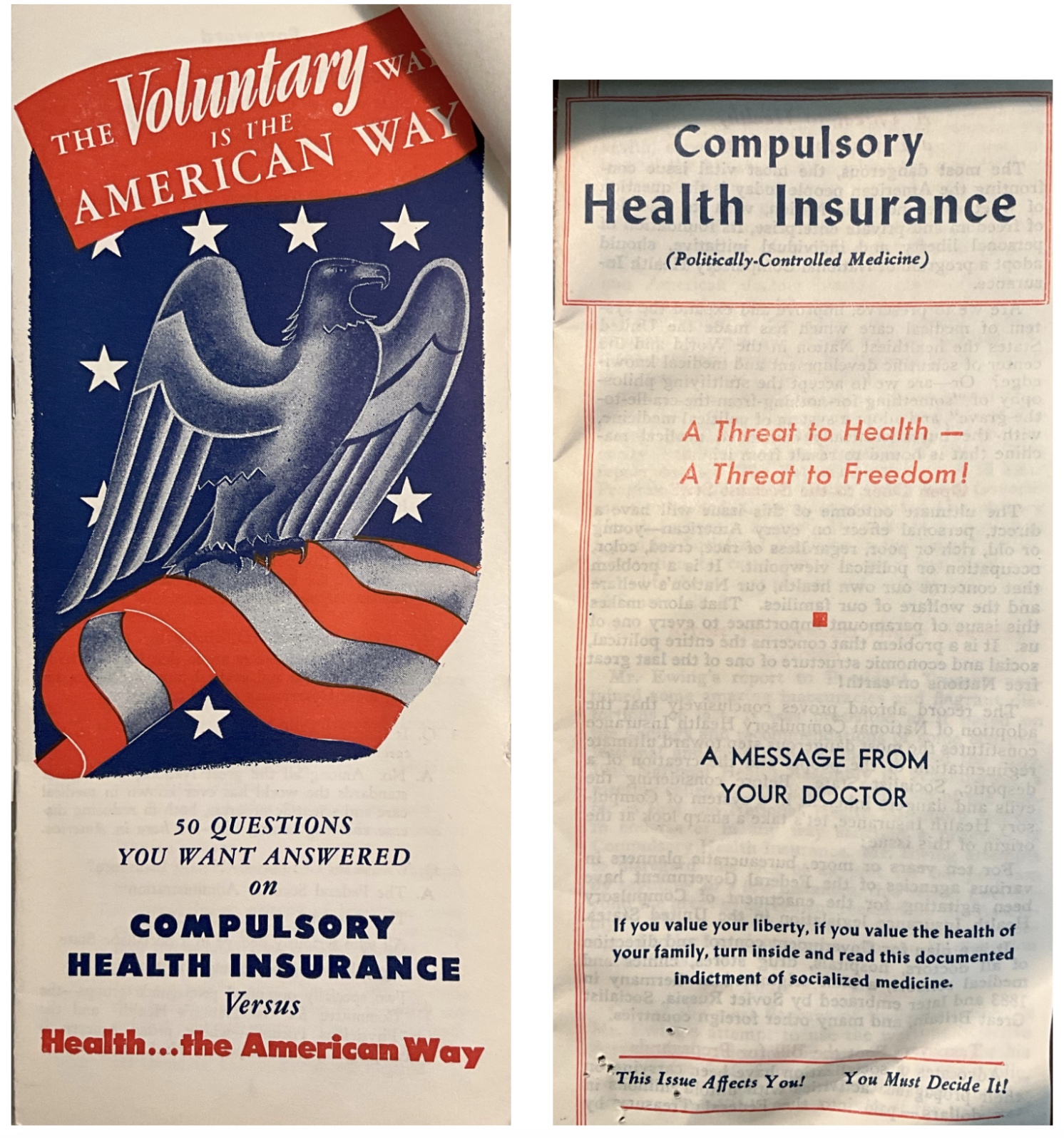
Notes: Figure plots two examples of pamphlets distributed by AMA-affiliated physicians during the campaign.
Source: Whitaker and Baxter Campaigns, Inc. archives.
Using several newly digitised data sources – including archival information from Campaigns Inc., digitised medical directories from the AMA, hospital directories from the American Hospital Association (AHA), invoices from the advertising firm Lockwood-Shackelford, and newspaper directories – we reconstruct the AMA-WB campaign intensity. The strategy outlined in campaign documents did not target specific places since it needed to react quickly, and modern statistical techniques of market analysis had not yet been developed. Furthermore, the market for medical insurance was far from saturated given that it was a new product. Instead, Campaigns Inc. relied on existing relationships and resources: tapping an advertising company it had used for years and pushing private insurance sales through the AMA membership. Empirically, we find that, conditional on factors that could plausibly influence demand for the private health insurance product – such as income, unions, and hospitals – campaign exposure is not correlated with the pre-existing (low) level of private medical insurance. Our primary outcomes of interest are enrolment in private health insurance, which we digitised from newly discovered Blue Shield reports, as well as public opinion data from Gallup Polls. Our analysis ends in 1954, when the federal government categorised payments for health insurance as tax-exempt, and corporate entities began to compete vigorously with Blue Shield.
We find that a one standard deviation increase in AMA-WB campaign exposure explains 20% of the increase in private health insurance enrolment during this period (Figure 2), and a similar decline in public opinion support for legislation enacting national health insurance. The results on public opinion are strikingly similar across a broad array of individual characteristics – however, respondents who had voted Republican in a prior election appear more influenced by the campaign, perhaps indicating the ideological framing appealed more to members of that party. We also find suggestive evidence that the campaign altered the narrative for how legislators described proposed health insurance legislation, using descriptors such as “compulsory” as opposed to “national” in text taken from the Congressional Record. Echoes of the campaign can also be detected in the phrasing of Gallup polling questions until questions on national health insurance ceased being asked as the issue moved off the legislative agenda. Taken together, the findings provide evidence for an underappreciated contributing factor as to why the US developed its unique and complex healthcare landscape. Although a historical paper, these findings may take on new significance given recent evidence on the importance of health insurance for improving labour productivity, reducing health inequality, and decreasing mortality (Baten et al. 2023, Del Valle 2015, Miller et al. 2021, Goldin et al. 2021).
Figure 2 Effect of campaign on private health insurance enrolment
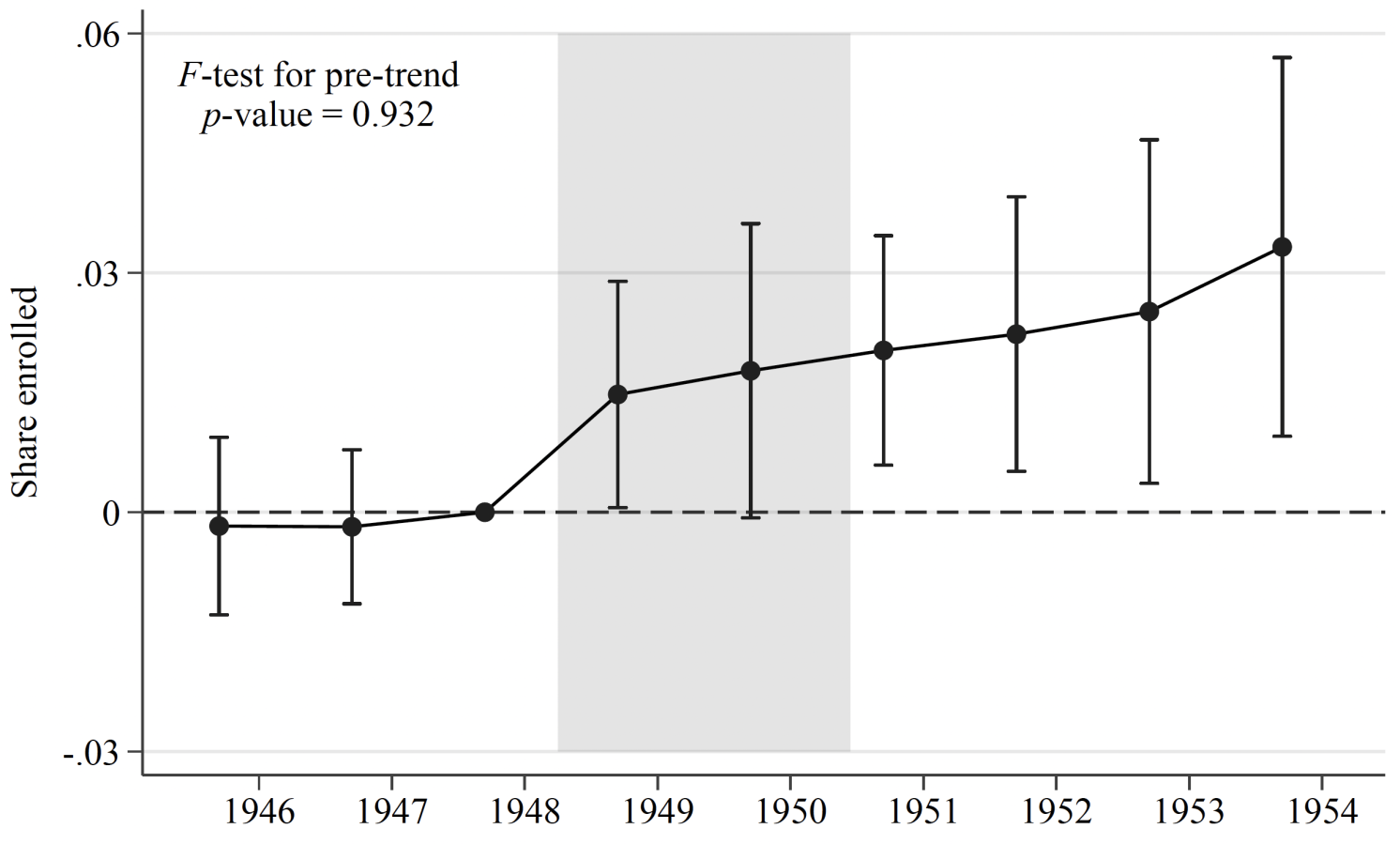
Notes: Figure plots event study coefficients of campaign exposure on private health insurance enrolment between 1946 and 1954. See Alsan et al. (2024) for further details.
Yet, why didn’t the US change course in later years? Our paper cannot easily tackle persistence empirically given the data limitations, but we offer several reasons for why the case for national health insurance was substantially weakened after the AMA-WB campaign. First, as middle-class Americans gained private coverage for themselves and eventually their dependents, the public option became less personally useful to many voters. Indeed, this was the explicit intent of offering a private option to begin with, according to campaign documents. Second, for-profit insurance firms increasingly entered the healthcare landscape: alongside pharmaceutical companies, hospitals, and specialist physicians, these groups continue to financially gain from and are a barrier to deviating from the status quo (Acemoglu et al. 2021). Third, the ideological argument that state involvement in healthcare invariably leads to socialism is still commonplace in the US – whenever reforms are proposed, the opposition’s response often explicitly refers to fears of socialism (see for example Gruber 2011). In other words, the narrative developed and promoted by the AMA-WB campaign remains firmly entrenched in US policy debates, with consequences for the nation’s health and the stability of insurance markets (Krugman 2021, Bursztyn et al. 2020).
See original post for references


Reposted on FB and took less than 3 min. to be whacked for community standards violation.
The communities at various social media outlets likely have many unexpected people, and maybe bots, doing their noting, bidding, hectoring, cajoling and manipulating. Their efforts at shutting down any substantive discussions have worked well enough to justify ongoing, say, program budgeting.
On the internet, nobody knows how many sick dogs there are.
The unspoken role of AI: feed a post to ChatGPT as a prompt and see if it self-censors.
Did your post explicitly mention NC and is that what they are censoring or the subject matter–just curious?
And we’ve talked about the above topic many times but not so much lately. And if one wants to step back our dysfuctional health care is not that different from our dysfunctional Pentagon and other areas that are supposed to be about defending the public welfare above all. Socialism suffered from an ideology that made everything social and capitalism from an ideology–Randian in a nutshell–that makes everything individual. And capitalism is so very much America’s ideology. So even if we had followed Britain and gotten national health care in the 1940s we would now, like Britain, be fighting like blazes to keep it.
It’s our ideology that is the villain and the fight for it against socialism consumed much of the 20th century. And in the end capitalism didn’t “win.” It’s just taking longer to collapse and may take the planet with it.
might try posting the original voxeu link, Roy.
back when obamacare was on the agenda and being argued about, i happened to have a lot of time on my hands to really dig in to healthcare(waiting on a hip replacement for 6.5 years,lol…)
this part of the story was perhaps the most infuriating…AMA being against healthcare, and actively mindf&cking the public to that end.
my own doctor of now 25 years(whom i consider a friend) started parroting this sort of thing, at first…but i set him straight,lol…he listens to me, and i used that shamelessly.
nowadays, and for the foreseeable future, i just do not have healthcare.
im ineligible for Disability(“work credits” went away long ago), and since i inherited 5 acres of salt marsh from my dad, my assets are too high for texas medicaid…or even SSI.
(and the other owners of that place dont want to sell, or buy me out)
and yet, all of my either wealthy or middle class family still insists that its stupidly easy to obtain public healthcare…that im malingering, or something…so the AMA’s efforts at propaganda and narrative control remain effective, all these years later.
i try not to think about it overmuch…because theres nothing i can do…but it still rankles.
It’s rentiers protecting their economic rents by any means necessary. The “socialism” bogey being an all-purpose Swiss Army knife in the propertarian tool kit.
I was 12. My father was a Taft republican and the Hudson valley where we lived was rock- ribbed republican at that time. National Health Insurance sounded like socialism to me and to most everyone around me and to the adults who had endured 16-years of misrule by “that man Roosevelt” and his successor with his awful Missouri accent.
Given the choice today of medicine in the jaws of parasitic corporatist finance or national health care, which would you choose?
When I was a postdoc at a major medical school in the Mid-Atlantic Region, I sat in the back row of several lectures presented to first-year medical students as part of my education. One was given by a then non-practicing MD who was working on the fine mechanisms of DNA replication in my home department. He had a reputation of saying everything he meant. The session was delayed for 15 minutes while representatives of the American Medical Association gave their sales spiel to a still-attentive captive audience of future physicians. When they left, their teacher for the day began by saying (I’m pretty sure this is the direct quote): “That is all well and good, but remember those people need you a lot more then you need them.” Then he gave an outstanding talk on the importance of topology and unwinding in DNA replication.
I’ve mentioned a book I have called “The Making of a Surgeon.” At the beginning of this book the author – William A. Nolen – dedicates it to his father and it reads in part-
‘When I was a boy he often said to me,
‘Billy, if you’re smart,
When you grow up you’ll be a doctor,
Those b******* have it made.’
And they did. So I find it ironic that those very same doctors, in an effort to cement their position in a lucrative field, ended up enabling the system to evolve where modern doctors have just become debt-ridden gig workers who spend more time on entering data into computer systems for insurance corporations and the like instead of their very own patients. The days of Marcus Welby, M.D. are long over and even if the US did have a national health system, it would be under constant attack like the US Postal Service is in the US and the NHS is in the UK.
“…ended up enabling the system to evolve where modern doctors have just become debt-ridden gig workers…”
First they came for the line workers, and I did nothing…
“They” being Big Capital.
Thanks to Yves for calling out the shameful role of some (but not all) labor unions. When we were tilting at windmills for single-payer in Ohio in the runup to the 2008 election, UAW was our staunch supporter. Andy Stern, on the other hand, screwed the poorest workers of his SEIU union and went on to become a cheerleader for Obysmacare.
Thanks for this. As Yves points out, there were a number of interest groups in addition to the AMA that mobilized against public health insurance for their own material or ideological reasons. But let’s not forget the central role of our neoliberal Democratic Party in heading off anything smacking of “socialism.” I remember well the Clinton fiasco. There was an excellent opportunity for real health care reform as Clinton entered office, with rapid cost increases leading to widespread demand for change, even among some big corporate interests. Of course there was furious lobbying against real reform, but there were political conditions for real progress as well. Instead we got the Clinton’s convoluted, HMO and Big Insurance based “managed competition” plan that emphasized, let’s see… oh yeah, “markets.” The corporate grift of that scheme wasn’t distributed widely enough, though, so it predictably crashed and burned.
The next such opportunity was when Obama came into office. NC readers don’t need a reminder of what happened there – the Heritage Foundation plan that had actually been the right-wing alternative to the Clinton effort in the 1990s. By the time Obama took over it was dangerous socialism.
I will never forgive nor forget our esteemed Senator/’representative’ Max Baucus ordering two nurses removed from ACA hearings – they had travelled from Montana to DC, on their own dime and time, to advocate for single payor national health. He had them removed by force by security. This was NOT January 6th behavior. Peaceful protest, free speech, advocating and looking for redress.
Way to go Max— here’s a plum- when you retire, ‘we’ will let you be the Ambassador to China.
Sheezus.
The American Way. I am reminded daily that I am one teeny square peg that slips through the nice full round holes of The American Way.
Then the Bernie Sanders’ campaign was vilified by countless op-eds in the NYT, Washington Post etc. proclaiming that Bernie was too radical for the American people who would never accept socialism. Mark Penn went so far as to say that his preferred candidate for president was Joe Manchin who was more in line with the American people! Obama then gathered support for Joe Biden who proclaimed that he was totally against any single payer program. Now we are supposed to support Biden as the lesser of two evils, What a country! We’re number one in everything!
And remember how the members of his own party stonewalled the “public option”, part of the menagerie of “rotating villians” that the party uses to stop any move leftward. During my lifetime that Heritage foundation proposal went from right wing, to Romneycare in “liberal” Massachusetts, to a leftist proposal by the Democrats that the Republican party tried to repeal over and over. I have seen the ratchet turn rightward by living it.
The United States is the only developed country where all citizens do not have health insurance. If universal health care is socialism, we need to rethink which side won the Cold War.
US is not a country or community, it’s a business, you are on your own. Pay your bills.
Yes, Caveat Emptor!
The other day, I was walking what has long been a rather hip stretch of bars and small shops near our downtown. Spitting distance from where the RNC will be, actually. It had been a while since I’d been there, but I was surprised and dismayed at the number of homeless people and drunks, in the middle of a hot day, including an elderly woman whom I had to wake to see if she was still alive. As I walked away, I saw a local shop-owner’s bumper sticker: “Nobody cares. Work harder.” It seemed appropriate. USA!
More to the topic: doctors collect rent by monopolizing knowledge capital; to further enrich themselves, they enable a bigger predator. Sick people are the smallest fish in this chain, and so don’t matter.
LOL. Thanks for that Oldtimer. The most truthful statement I’ve heard today.
And we are proud of it! I should add that my primary care doctor, who is a libertarian, believes that the whole mess would be fixed by eliminating Medicare!
The 2012 Jill Lepore (Harvard historian) piece (which I have linked to several times here on NC) mentioned in the present piece is most informative (and depressing). It starts with the fight against Upton Sinclair’s campaign for CA governorship in 1934 and moves on to other (largely successful) efforts to propagandize the population. It always makes my day when I learn something more about how and why the world we live in is so ƒ¨ç˚´∂ up.
The Lie Factory
Sinclair wrote about it in his book, I, Candidate For Governor, And How I got Licked.
When Sinclair unexpectedly won the Democratic nomination for Governor, the mainstream Dems ran a spoiler candidate to sink him. The split begun then between the business and left wings of the California Dems continues today.
His movement, End Poverty In California (EPIC) should not be forgotten. At one point, a third of the California Assemby members were in the EPIC caucus.
Thank you for the link! The Lepore piece is well worth the time.
And the most recent fudge by the government is cutting back on Medicare coverage for various standard procedures and lab work. I just got a notice that Medicare might not pay for thyroid panels in future. Which is so stupid as to be counterproductive since maintaining a good thyroid profile is essential for good health. They appear to be glossing over this blatant incompetence with a new promise of a COLA increase for social security payments. No one as yet has divulged how much the Medicare deduction has risen to. But since it is an election year that won’t happen before the “election.”
Is that Medicare or Medicare DisAdvantage? I haven’t gotten any notice.