Yves here. This article shows that the robustness, or lack thereof, of the elderly is starting to get official attention. The authors constructed a frailty index, using data from the Health and Retirement Study and the English Longitudinal Study of Ageing. which frustratingly the authors do not indicate precisely what the information consists of: is it all objective measures or does it include self-reporting? Has there been an attempt to validate any self-assessments?. Their description:
Frailty indices aggregate information across a range of indicators (e.g. medical conditions, ability to perform certain activities) and are scored from 0 (low) to 1 (high) to reflect a person’s physiological (both mental and physical) frailty.
The reason for taking interest is that efforts like these might affect policy, and well done, they could or should also affect medical practice. However, the way the medical part is becoming a pursuit of anti-aging, which often includes big ticket quackery, and questionable trickle-down to regular patients. Admittedly, as some readers pointed out yesterday in the active discussion of Nancy Pelosi’s hip fracture, many older people and even not so old people get marching orders as to what to do to improve their health, and even with personal attention, like regular visits from physical therapists, many refuse to comply.
This piece also unintentionally hints where these tendencies may be going. It cites the new hot weight loss drugs, the GLP-1 agonists like Ozempic, as lowering biological age. But is there any all-cause mortality data on long-term use? I don’t think there is yet that sort of data. And I do not know how often patients decide to stop using them, but they seem to gain the weight back when they do. I have read that some, perhaps even many, become voraciously hungry, so it could even be that some wind up worse off.
In terms of longevity and biological age effects, one would think that the fat and obese losing weight would be a clear health benefit: reduced load on the heart and joints, better blood sugar readings and so lowered risk of diabetes,.
But one of the side effects of GLP-1 agonist use is Ozempic butt and Ozempic face, which the results of internet searches depict as the result of fat loss. But that is not fully consistent with IM Doc’s findings. Via e-mail:
I am seeing large numbers of formerly obese patients who are now looking like Icabod Crane – massive facial muscle and arm and thigh muscle loss. Thanks to Ozempic et al.
Recall the frailty framing, that that is the defining aspect of biological versus calendar age.
Consistent with that I had a very very good endocrinologist back in the day. Eventually as many did he converted his entire practice to monthly (high) fee anti-aging.
He went to a lot of anti-aging conferences.
At one, the doctors were given a list of 20 metrics, like VO2 max, a1c, resting pulse, LDL, blood pressure, testosterone, triglycerides, BMI, bone density, kidney function measures and so on.
They were asked to guess the one that best predicted biological age as opposed to physical age.
The two best in reality:
1. Strength
2. Muscle mass
So if GLP-1 agonists are having the effect of reducing muscle, are they necessarily as beneficial as depicted? Admittedly, when body builders are dieting down to minimize their body fat for contests, they do lose muscle mass too. But they do not lose strength. This issue bears watching.
And will other new wonder drugs be scrutinized for their impact on biological age as well as all factor mortality?
By Rainer Kotschy, Visiting Scientist Harvard T.H. Chan School of Public Health; Postdoctoral Fellow National Bureau Of Economic Research (NBER); David Bloom, Clarence James Gamble Professor of Economics and Demography Harvard University; and Andrew Scott Director of Economics Ellison Institute of Technology; Professor of Economics London Business School. Originally published at VoxEU
Analysis of population ageing is typically framed in terms of the number of years lived since birth. This column uses data from studies on physiological functioning in the US and English populations aged 50 and older to show that for policy and research purposes, the reliance on chronological age is at best incomplete and at worst misleading as it provides only limited information about the ageing process. Improvements in how we measure ageing and our understanding of how it affects people and the economy are needed if we are to adapt to the reality of longer lives and overcome the challenges posed by population ageing.
Populations worldwide are growing older. Falling birth rates, increases in life expectancy, and the progression of large-sized cohorts to advanced ages are leading to both rising proportions and numbers of older people. For instance, in Japan, one of the countries furthest along the demographic transition, the proportion of the population aged 65 and older rose from 4.9% in 1950 to 29.6% in 2020 and is projected to reach 37.5% in 2050 (United Nations 2024).
Population ageing is seen as a major economic challenge, adversely impacting the growth of GDP and the sustainability of public finances (Smith et al. 2015, Bloom 2019, Goodhart and Pradhan 2021, Kotschy and Bloom 2023a, Cooley et al. 2024).
Analysis of population ageing is typically framed in terms of chronological age – i.e. the number of years lived since birth. This framing has multiple advantages: chronological age is readily understood, easily measured, widely available, and commonly defined across both individuals and over time. These features, along with rising numeracy and literacy, led to the introduction of chronological age in regulations and bureaucratic measures (e.g. compulsory schooling ages, restrictions on child labour, and the right to marry) in the UK and the US in the 18th and 19th centuries (Thomas 1976, Chudacoff 1989).
The widespread use of chronological age in the context of population ageing came with the introduction of modern pension systems. In 1889, Germany launched the world’s first modern pension system with a retirement age of 70, later lowered to 65 (Mierzejewski 2016). The use of chronological age to define the ‘old’ was a natural extension of this bureaucratic standardisation. The legacy of this approach is evident in how we measure the existence and extent of population ageing today.
In recent work (Kotschy et al. 2024), we show that for policy and research purposes, the reliance on chronological age is at best incomplete and at worst misleading. That is because chronological age – the mostly widely used indicator of ageing – provides only limited information about the ageing process.
The underlying problem is that chronological age is not revealing about how we age. Instead, its use is justified as a proxy for a variety of underlying measures capturing different dimensions of ageing such as biological resilience, cardiovascular fitness, cognitive functioning, and wisdom. Chronological age can be a useful shorthand for these multiple dimensions, but it does not directly measure or illuminate the key mechanisms and characteristics of the ageing process.
Ageing plays a central role in multiple economic processes, behaviours, and outcomes. Examples are life cycle issues involving consumption, savings, labour supply, and education, as well as preferences and macroeconomic issues of productivity, innovation, and growth. However, as we show, chronological age per se is rarely the relevant variable of interest. For instance, in issues of labour supply it is often health and declines in physical and cognitive capacities that matter (Blundell et al. 2016). Similarly, when it comes to saving, what matters is how much remaining time a person can expect to live (what Sanderson and Scherbov 2019 call ‘prospective age’) and not how long they have already lived (Strulik 2023).
The usefulness of chronological age for policy and research depends on it having a stable and well-defined relationship with key dimensions of ageing, such as physiological functioning. But if the aim is to provide insights as to how to adapt to increased longevity (Scott 2024), chronological age will be an unstable and imperfect proxy for the key dimensions of ageing. For instance, Kotschy and Bloom (2023b) show how shifts in physiological ageing, as measured by changes in population age structure and longevity, can lead to more optimistic projections of GDP growth under population ageing due to expansions of labour potential into the older ages.
To explore the extent to which chronological age reliably approximates population ageing, we used data from the Health and Retirement Study and the English Longitudinal Study of Ageing and constructed frailty indices (Mitniski et al. 2001) to measure physiological functioning in the US and English populations aged 50 and older. Frailty indices aggregate information across a range of indicators (e.g. medical conditions, ability to perform certain activities) and are scored from 0 (low) to 1 (high) to reflect a person’s physiological (both mental and physical) frailty. As summary measures of ageing, they are increasingly popular in economics literature (e.g. Abeliansky and Strulik 2018, Hosseini et al. 2022, Old and Scott 2023).
Our analysis spotlights three reasons why chronological age cannot be expected to reliably approximate physiological age: heterogeneity, malleability, and multidimensionality of physiological functioning.
With respect to heterogeneity, people of the same age differ appreciably in physiological functioning, and increasingly so. Figure 1 shows that frailty tends to rise with chronological age; however, there is enormous variation across people. The healthiest 10% of the population at age 90 are close to the level of frailty displayed by the median 50-year-old, and the healthiest 25% of 90-year-olds are in better health than the least healthy 50-year-olds. In fact, chronological age accounts for less than 10 percent of the variation in frailty in bivariate regressions (Kotschy et al. 2024, Table 1). This within-group variation means that chronological age alone is a rather unreliable indicator of a person’s physiological functioning.
Figure 1 Frailty distribution in the US by chronological age
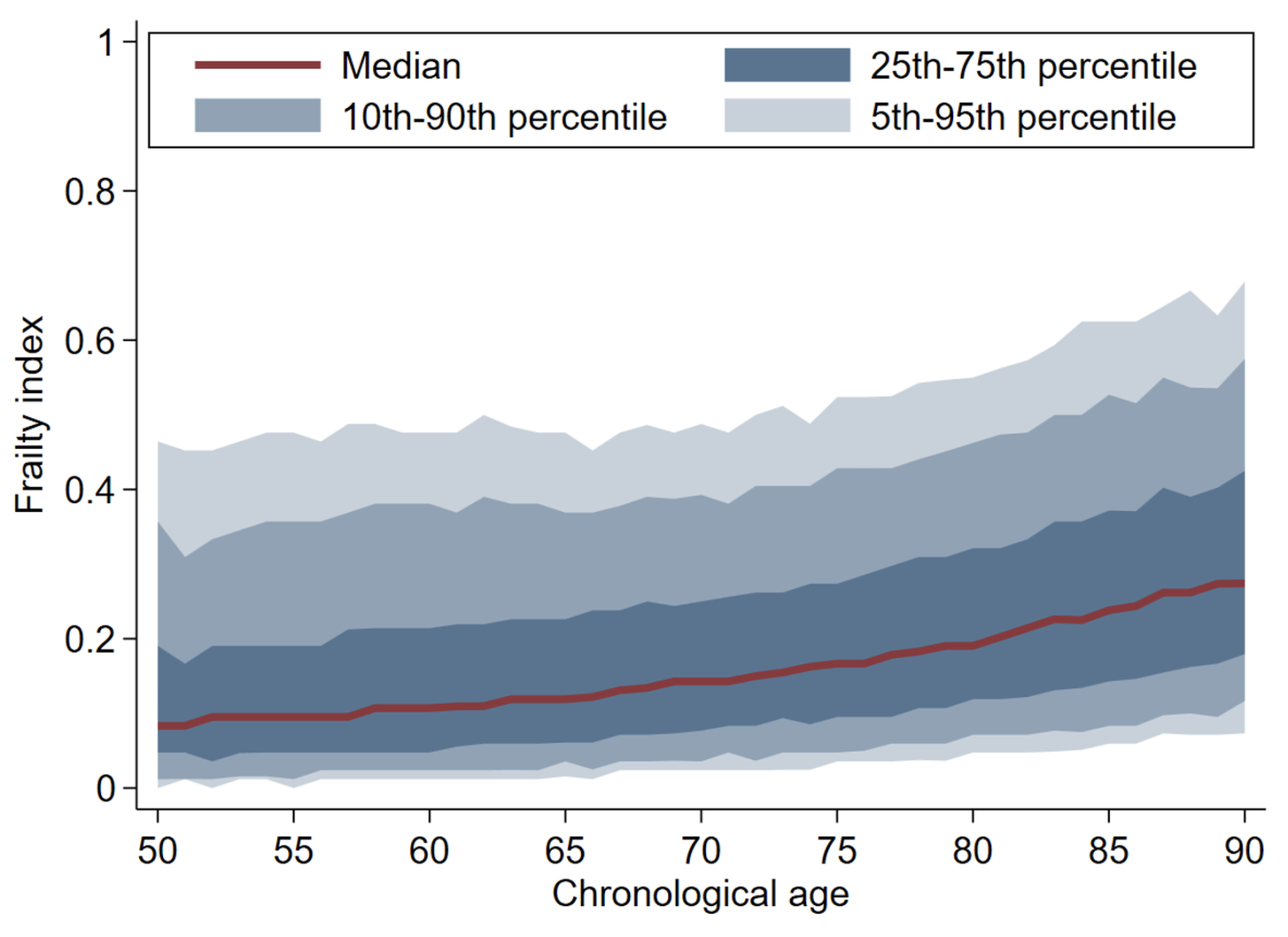
Note: Authors’ calculations (see Kotschy et al. 2024, description of Figure 1a). This figure shows patterns and trends in physiological functioning, as measured by the frailty index, in the US conditional on chronological ages for different percentiles.
Malleability refers to the fact that the rate at which people physiologically age can change over time. This phenomenon, reflected in popular phrases such as “70 is the new 60”, might become even more pronounced if new therapeutics emerge exploiting advances in the biology of ageing (Campisi et al. 2019); noteworthy examples are GLP-1 agonists and new vaccines. It could also result from improved living standards and related changes in consumption toward healthier diet and increases in physical activity.
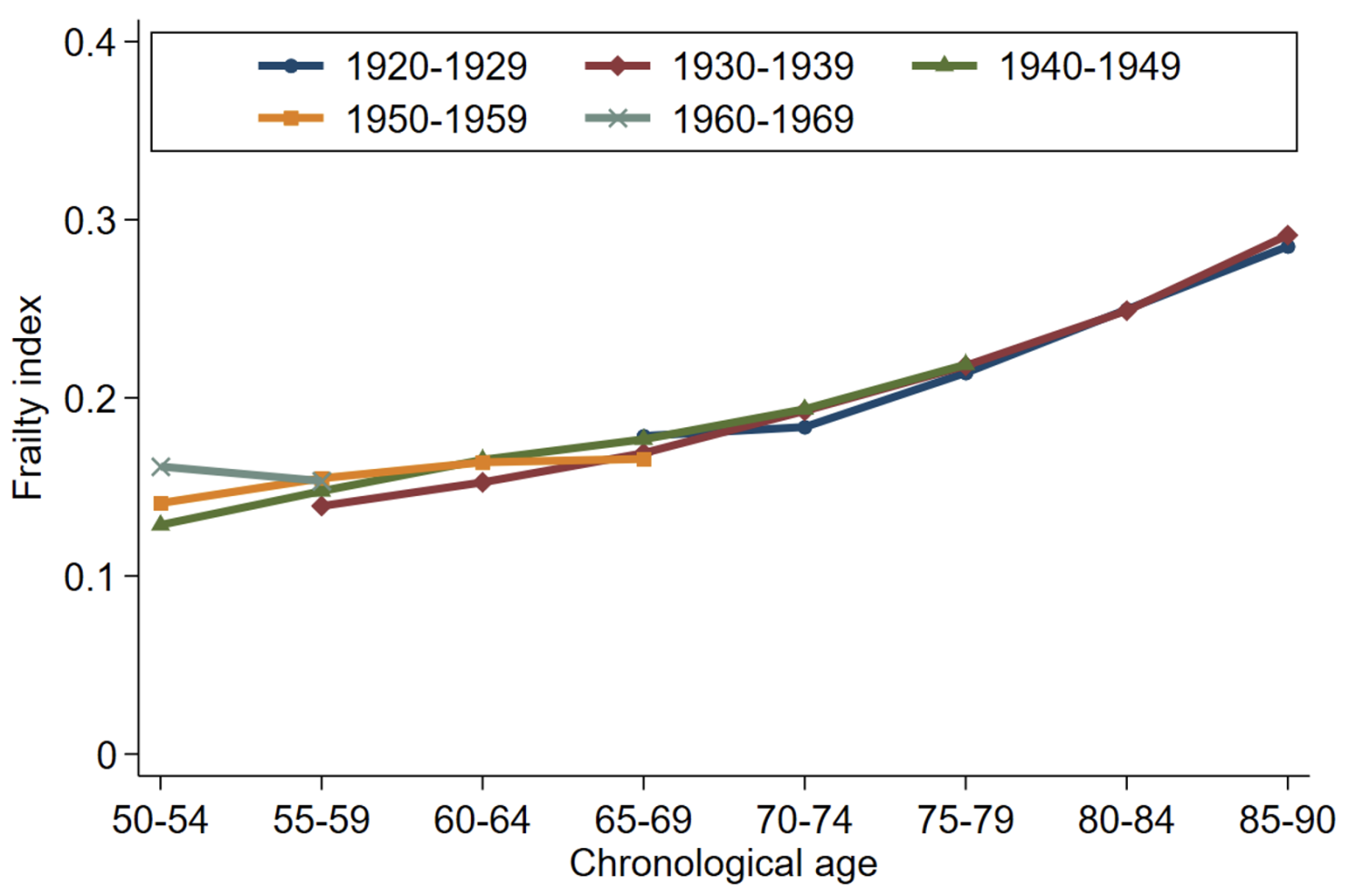
Figure 2 shows frailty indices for different birth cohorts in the US (Panel a) and England (Panel b). Conditional on chronological age, average frailty levels have decreased in England but not in the US. This observed malleability implies that population measures of chronological age will not adequately reflect the degree of population ageing over time and across countries.
Figure 2 Average frailty by chronological age and birth cohort in the US and England
a) Average frailty by age and cohort: US
a) Average frailty by age and cohort: England
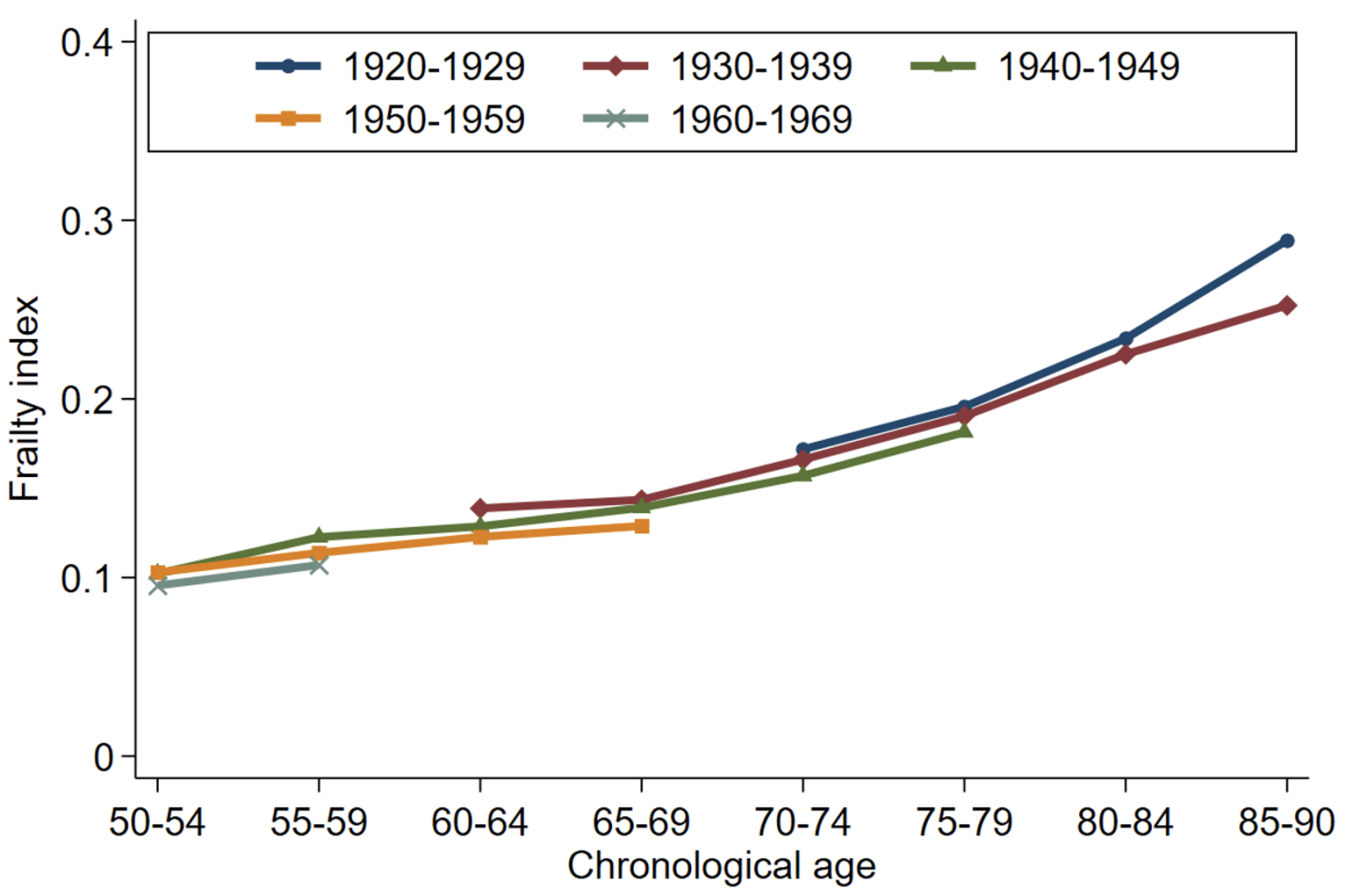
Note: Authors’ calculations (see Kotschy et al. 2024, description of Figures 1c and 1d). This figure shows patterns and trends in physiological functioning, as measured by the frailty index, in the US and England conditional on chronological ages across five birth decades, covering the 1920s to the 1960s.
The multidimensionality of ageing represents another reason that chronological age might not accurately approximate physiological functioning. If different domains of physiological functioning – such as locomotor, cognitive, and sensory functioning – show different trends, the reliance on median age or the proportion of the population aged 65 and older will likely conceal differences in the trends and patterns of the underlying domains of physiological functioning.
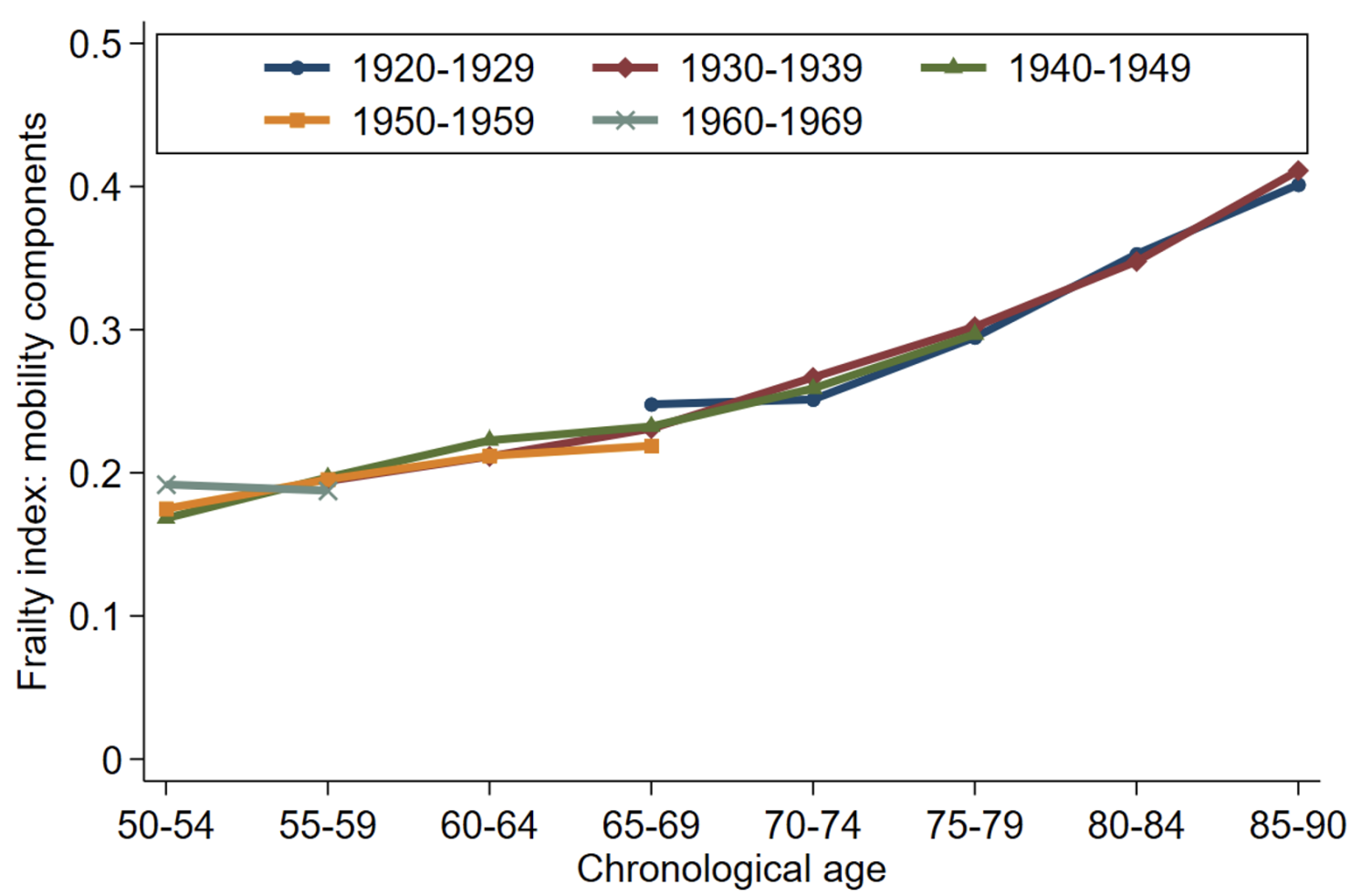
Figure 3 shows that the mobility components of the frailty index have a steeper age gradient than the psycho-cognitive components. Moreover, average frailty levels have somewhat decreased across birth cohorts in the psycho-cognitive domain but not in the mobility domain. The implications of population ageing therefore differ substantially depending upon which dimension of ageing is important, something that chronological age will not naturally capture.
Figure 3 Age patterns in physiological functioning across different domains in the US
a) Mobility components
b) Psycho-cognitive components
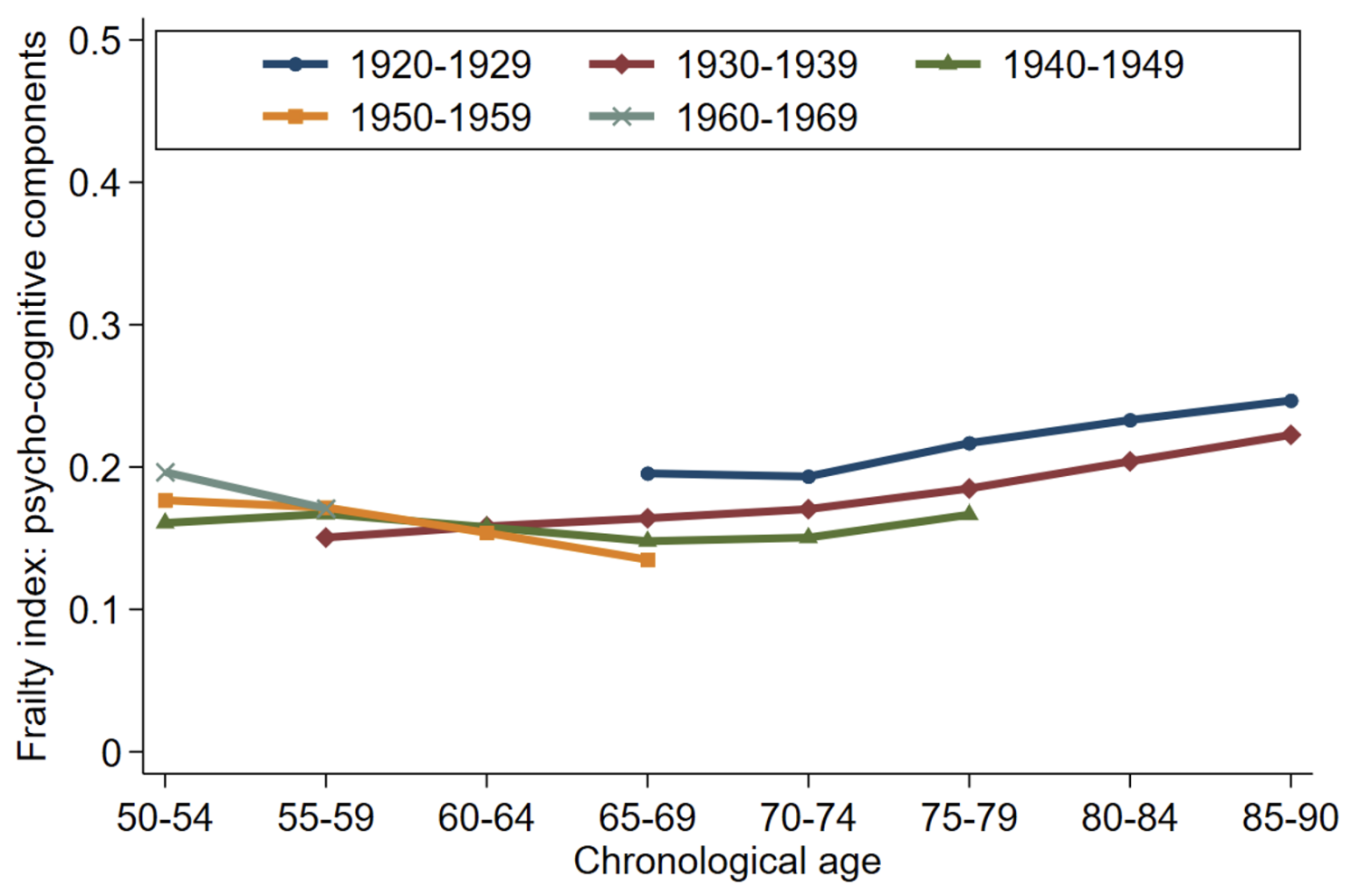
Note: Authors’ calculations (see Kotschy et al. 2024, description of Figure 2). This figure shows age patterns in physiological functioning, as measured by a frailty index, in the mobility domain (Panel a) and the psycho-cognitive domain (Panel b) across five birth decades, covering the 1920s to the 1960s.
These three problems – heterogeneity, malleability, and multidimensionality – all point to difficulties in using chronological age as a measure for ageing.
Our empirical analyses underscore the real-world nature and importance of these difficulties. We analysed data from the US Health and Retirement Study to compare the predictive power of chronological age and physiological functioning for key economic behaviours and outcomes (including employment, working hours, hourly wages, volunteering, help to others, life satisfaction, out-of-pocket medical spending, and recent overnight stays in a nursing home or hospital).
Our results document that (1) all variables, except for hourly wages, are influenced by physiological functioning (as measured by a frailty index); (2) for most outcomes chronological age and physiological functioning have independent effects; and (3) the inclusion of a frailty index barely affects the estimated effects associated with chronological age (Kotschy et al. 2024, Table 2). The upshot of this analysis is that chronological age does not reliably account for the effects of physiological functioning on economic behaviour and outcomes. In fact, the effects chronological age picks up are distinctly different from the effects picked up physiological functioning.
Overcoming the challenges posed by population ageing requires a precise understanding of how we age, the economic consequences associated with ageing, and how to achieve better health and economic outcomes. Chronological age has the virtues of simplicity and regularity. However, the heterogeneity, malleability, and multidimensionality of physiological functioning among people at the same chronological age limits the usefulness of chronological age in research and policy settings.
Further work is much needed to improve the measurement of ageing and our understanding of how it affects people and the economy if we are to adapt and adjust to the reality of longer lives and overcome the challenges posed by population ageing.
See original post for references


Start a better diet today. Eliminate inflammatory items like processed foods, seed oils and those grains that have pesticide forever chemicals. You can’t pick your relatives but you can be picky about the food you consume. Read the labels and learn to reject the foods laden with chemicals.
Lift weights, even light ones, and walk. See, that was easy. The longevity journey starts with organic first steps.
That sums it up! You are what you eat. I gave up 95% of ultra-processed gunk, increased fat and protein and fresh spinach, and cut down on carbohydrates. I lost weight without going on a diet – I just changed my diet and was never hungry. I did have an interval of medical treatment in which I lost too much weight, but I am now back to high school level, which was some time ago. Walking, not strolling, stresses the long bones of the legs appropriately and stimulates osteoblasts (bone building cells) over osteoclasts (bone resorption cells). Ditto for hand-held weights, 2-5 pounds each more than enough. The muscles get a workout, too. Working on your plank every day is another effective exercise that does not place too much stress on the body while strengthening the core beyond all expectations, in my experience. This is not difficult, but Big Medicine doesn’t have a role, so it is “suspect.”
GLP-1 receptor agonists are ingenious interventions for the treatment, and eventual resolution, of Type 2 diabetes as part of a holistic readjustment for the patient. Period. Artificially altering global metabolism is never a good thing.
Sibling who worked for decades as a visiting physical therapist told me that all, 100%, of the centenarians she encountered had been gardeners earlier in life. She interpreted this in terms of the way that working the soil helped to preserve functional strength.
I imagine that there might also be 2nd order effects in terms of mental health, stress reduction, and the feedback of those to general bodily well-being.
“…been gardeners earlier in life.”
Probably also related to was IM Doc wrote recently, namely that core strength, strengthened by activities like gardening, is a major factor in avoiding fractured hips, etc.
Time spent gardening is never wasted.
Said by destressed people for years.
Time flies, zoning out with planting, pruning, weeding and even fiddling around with sprinklers.
That last one might bring occasional frustrations while anticipating results.
Patience, patients.
Also, gardening gets you rolling in the “fermented” soil. Fermentation turns biomass into soil. The microbes that gardening people ingest and get on their skin, creates a diverse microbiom- inside and outside of said gardener!
This is why fermented food is so so so important for our heath. Kimchi, sauerkraut, yogurts, kvas, etc etc
We made and ate lots of fermented foods before the neo-miracle of refridgeration. Now, we throw food out if it is past it’s use-by-date or looks funny. We refridgerate or freeze everything.
……and, as a result of our “microbe-freeness”, we end up looking like death warmed up.
Admittedly, when body builders are dieting down to minimize their body fat for contests, they do lose muscle mass too. But they do not lose strength.
Yes they do. . . and body building is not a strength sport, its basically modelling. If you look at Ironman competitions or Powerlifting, you see some people with significant body fat (because the reverse is true as well), especially in the highest weight categories because there is no performance downside the way there might be if you can cut down to a lower weight class.
Part of the reason performance drugs are so prevalent in body building is to prevent/minimize the loss of muscle mass from severe calorie restrictions (some of these people get down to 4 to 6 percent body fat, pushing the limits of where you reach organ failure). If you look at natural body building competitors vs. better-living-through-chemistry “normal” body building, you can really tell.
As your body gets down from 10 percent to ~3 percent body fat (at which point your organs begin to stop functioning properly and death quickly ensues), your body will increasingly turn to metabolizing muscle to protect itself unless you are getting horse doses of testosterone. I think there were some studies on Army Rangers that at about 6 or 7 percent, the body just starts practically eating muscle almost exclusively.
Muscle mass is only one component of strength– there are factors like muscle recruitment–but it is very strongly correlated.
Yes, building muscle strength is different than building muscle size. Body builders use single muscle movements to develop size. Athletes use whole body movements and work muscle groups to develop power/speed/explosiveness. (Which also increases muscle size, but in coordination with whole body movement.)
The reason for ‘Ozempic Butt’ is there is no underlying muscle (gluteus) mass and so the fat-stretched skin sags (especially if you are middle-aged).
It takes serious effort to develop/sustain muscle mass (even if you are young). You must progressively increase the weight lifted to challenge the muscle to induce muscle growth. Muscle growth requires protein in the diet (more than you imagine). One can begin improving muscle mass using your body weight; simple squats, single-leg lunges, sit-ups, push-ups, pull-ups. But a weight-room with an instructor and access to progressive weights is the best option. Injury will delay your progress.
I’m in a college weight-room three days a week. I workout with college athletes and regular students—only those who avoid their cell phones and the ‘chat impulse’ make progress.
As for longevity, the strongest correlation is between VO2 max and muscle mass. Maintaining these two gets harder as you get older: muscle joints/tendons get balky, balance diminishes, running/biking (aerobic activity) gets harder (dangerous). An organized gym workout is best for newcomers/elderly (treadmills/stat-bikes/ weight machines) and certified trainers.
The road to better health requires a comprehensive plan.
Add:
Learn to swim to maintain aerobic fitness. There is also a “zen” component to the activity. Start now! (I’m off to the pool at noon.)
I’m 53 and have been vegan for 19 years and did not get vaccinated. My GP is always shocked at how good my bloodwork is every year. Used to do a lot of yoga but it dropped off during the pandemic.
Decided recently I needed to up my activity levels so I started boxing lessons in August (the real gritty NYC deal). After about a month of soreness I’m keeping with a guy that’s 17 and another that’s 23 (both in excellent shape).
I’m waiting for the appropriate moment to drop the age bomb on them. :)
I was a strict vegan (for ethical reasons but it was health food) for 19 years and ended up with cardiac calcification that was probably due to lack of K2. It is hard to get enough K2 as a vegan if you don’t supplement; that wasn’t known when I was vegan. I only found out due to a scan for purposes of donating an organ to a sick relative (I couldn’t because of the calcification). You might want to make sure you get enough K2, and consider asking your doctor if a cardiac calcification scan would make sense. I was in fantastic shape otherwise when I found this out, so it’s not like there are symptoms.
For yours truly, its all about channeling Sisyphus, in that all I do for exercise is walk up trails that net me 1,500 to 2,000 feet of elevation gain typically, only to give it all back on the way down.
One thing i’ve noticed about most people is they only walk on dead flat surfaces pretty much, and i’m dodging rock obstacles a decent amount of the time on the trail, so uneven surfaces keep me limber.
Found a new trail on BLM land here, it’s one friends call ‘the straight up’ trail, 1,500 feet of elevation gain in about 2 miles.
It’s so steep that it is also a challenge walking back down.
…and the natural setting with fresh air, no-engine noise, and vista’s ‘to-die-for’ induce repetition. Lucky you.
What makes my environs perfect for the job is there are low altitude trails for the winter and spring and then I switch to high altitude trails, so there’s always a nice variety.
Walked to Marble Falls in Sequoia NP yesterday with 3 friends, and we generally never walk faster than we can talk, so add a lot of conversation to the mix as well.
People want to live forever and be forever young. Hah! My friend says he will be attending his grandfather’s 100th birthday. One beer a day and a cigar on occasion and no exercise or diet routine is the old guy’s habit . For some, luck and genetics is all it takes. For most, IMO, it takes some planning and training. In my age cohort, 75, unscientifically, the ones still alive, I would estimate 80% have some major issues and almost all have a current issue of some sort (or one on its way).
So taking a look at the 20%, let them be called outliers, insiide that group there will be a subset of even healthier outliers. Over time this group will get further culled, so on and so forth. I would bet most of these outliers started some sort of program when they were in their forties (or sooner). I know a woman, latte 70’s, who is in a rage that RFK Jr. could ban ozempic. I said that maybe not eating processed foods, sugar, & salts and getting a little exercise might be OK. That ended the conversation
The problem in the US, is that our society doesn’t give a damn about the population’s general health. Having travelled around the world during the last ten years (mostly Asia/Central Asia), the groups with the most heavy weights were in the US, Mexico, and Mongolia. Again, unscientifically, one comes to the conclusion that people in the US get crap food (most people in the the ‘east’ seem active, so it’s presumable that food is more a factor than exercise). In the US, people seem to put work ahead of quality of life and appearance before fitness. It’s a crap formula. What happens is people are working longer, dying sooner, or living longer but with less quality of life. The trick seems to be to stay active but do do it smart. The people who say, post 70 , that they feel young (like a Pelosi) should get an xray of their bones. The ones who think that they can keep up with the ones half their age,, (like a Biden) are in my opinion, hypoxic. In any case aging is a process of adaptation. Blood pressure and blood sugar monitors should be available to people in their 30’s so they can fully understand how the process works.. Prioritizing objectives is not rocket science.
the “latino paradox”, imho lends credence to your thoughts. mexicans and central americans coming here were observed to be among the healthiest people in the country, largely (it was assumed) due to their diet, largely beans, non-gmo corn tortillas and vegetables. after some time here and americanization of their diet they are among the least healthy.
Multiple relatives made it into their late nineties. They didn’t do anything special – maintained a social life with neighbors and fellow church members, gardened and ate a lot of vegetables, walked the neighborhood, kept up with current events but maintained a positive outlook anyway, maintained healthy body weight. Genetics? Lifestyle? Unpolluted small town air?