Yves here. Even with having been attentive to Covid studies and news, KLG’s overview contains quite a few information nuggets that were new to me. For instance, the UK quickly started taking blood samples of ~100,000 patients every 5-6 weeks in what it called the REACT survey to assess, among other things, prevalence of Covid (recall it can be asymptomatic) and whether it was mutating. Commentator were looking at the decline in antibody levels over time among the infected as a proxy for how long immunity lasted. However, KLG describes below that antibody levels “do not correlate with protection from infection.” So the lay and even the professional press has misreported this issue.
KLG also explains, long form, why using only the spike protein may not have been the best approach for a vaccine. Note that KLG also stresses the lack of durable immunity to coronaviruses and what that implies for disease prevention and treatment. This is not even remotely new news; we stressed that from the very outset. Yet he points out how that basic issue has been bizarrely ignored in public health responses.
KLG’s introduction:
COVID-19 did not appear out of nowhere. SARS (2002) and MERS (2013) were first, but the original serious coronavirus disease was caused by Infectious Bronchitis Virus in chickens. The biomedical responses to COVID-19 did not fully take into account previous knowledge of coronavirus disease, especially that durable immunity to coronaviruses is basically a unicorn. Hindsight is often 20:20, but had the scientific and political establishments paid more attention to the known pathobiology of coronavirus disease over the past five years than the bright shiny prospect of vaccines, our collective responses might have been more effective. Perhaps they will improve next time. And there will be a next time.
By KLG, who has held research and academic positions in three US medical schools since 1995 and is currently Professor of Biochemistry and Associate Dean. He has performed and directed research on protein structure, function, and evolution; cell adhesion and motility; the mechanism of viral fusion proteins; and assembly of the vertebrate heart. He has served on national review panels of both public and private funding agencies, and his research and that of his students has been funded by the American Heart Association, American Cancer Society, and National Institutes of Health
COVID-19 (agent of disease: SARS-CoV-2) did not appear ex nihilo in late 2019. It was presaged by the outbreak of SARS (Severe Acute Respiratory Syndrome) in 2002 and by MERS (Middle East Respiratory Syndrome) ten years later. SARS (SARS-CoV) spread from Guangdong to Singapore and Toronto by early 2003 but was contained by rapid and effective public health measures. Nevertheless, 774 patients in a population of 8,098 reported cases died (9.6%). The death rate for MERS (MERS-CoV), which is not as transmissible as SARS, was ~34% in a population of about 2,600. The death rate for COVID-19 is much lower than for either SARS or MERS, but the current pandemic has killed more than 20 million people worldwide. All three diseases are caused by coronaviruses, which have been recognized as viral pathogens in vertebrates since 1949 and probably earlier.
What follows is an attempt to put COVID-19 in context based on a focused consideration of a coronavirus literature that has become quite large (and intractable) in the past five years. My priors are that the only way to address a scientific problem correctly is to go back to the beginnings so that the foundation of current research is as strong as possible. In my experience in biomedical science, this is the only way to make significant discoveries, small or large. Otherwise, the scientist is only placing bricks on a pile with little thought for how they fit together. [1] This essai is only that, and attempt, and I expect more complete coverage to emerge in the next few years from several perspectives, scientific and political.
We begin with the response to SARS from the perspective of an expert on coronavirus disease in poultry. The first coronavirus disease in vertebrates is caused by what is now known as Infectious Bronchitis Virus (IBV): Severe acute respiratory syndrome vaccine development: experiences of vaccination against avian infectious bronchitis coronavirus (D. Cavanagh, 2003; Institute of Animal Health, currently the Pirbright Institute). Until SARS, human coronaviruses caused only mild upper respiratory tract infections. This paper is representative of several published after the SARS outbreak that addressed how previous experience with the IBV should be useful in dealing with serious coronavirus disease in humans. This review is especially relevant because it concentrates on vaccines against coronavirus disease, and the primary response to COVID-19 has been vaccination.
Coronaviruses have been placed into four taxonomic groups:
- Group 1: Human coronavirus 229E, Feline infectious peritonitis virus
- Group 2: Human coronavirus OC43, Murine hepatic coronavirus
- Group 3: Infectious bronchitis virus (IBV)
- Group 4: SARS-CoV, SARS-CoV-2, MERS-CoV
These viruses are divergent and some cause more serious disease than others. The most well studied coronavirus prior to the SARS outbreak of 2002-2003 was IBV, primarily because it presents a very serious problem in chicken production in Concentrated Animal Feeding Operations (CAFOs). CAFO-based poultry production began in the 1950s in the United States.
IBV pathobiology has much to teach us about coronavirus disease and the role of vaccines in industrial chicken production. These lessons include:
- The best practice is to vaccinate newly hatched broilers on Day 1.
- Protection against disease lasts a short time, and this may require re-vaccination for chickens that are grown longer than 4-6 weeks before slaughter.
- Spike protein (the viral envelope protein that looks like the “crown” in electron micrographs of coronaviruses) may be used as the immunogen for vaccines, but minor divergence in IBV spike variants yields poor cross protection. As a reminder, the exterior spike protein segment is the expression construct in the SARS-CoV-2 mRNA vaccines.
- Circulating antibody levels do not correlate with protection from infection.
- The schedules required for protection of chicken “flocks” in CAFOs are not cost-effective, which requires rigorous infection control in large chicken houses that may accommodate tens of thousands of birds. [2]
Thus, based on experience with IBV vaccines (p. 568): “Application of a SARS vaccine is perhaps best limited to a minimal number of targeted individuals who can be monitored, as some vaccinated persons might if infected by SARS coronavirus, might become asymptomatic (shedders) of virus, thereby posing a risk to non-vaccinated people.” This research on IBV shows that coronavirus vaccines can be developed, and they elicit an immune response. However, this immune response does not correlate with protection from disease, nor is the immune response durable. Cavanagh’s conclusions are particularly relevant in 2025. As Cavanagh put prospectively sixteen years before COVID-19:
If there were a resurgence of SARS in humans (SARS-CoV-2 qualifies) one would anticipate that the authorities would rapidly put into operation the various surveillance and control measures that proved successful in early 2003. If vaccines had been developed, vaccination might be included, especially for healthcare workers and contacts in the wider community. Coronaviruses can establish persistent infections (in which the virus can evolve) in at least a portion of their hosts, resulting in chronic asymptomatic shedders, with subsequent problems for containment of th disease. For this and other reasons, a decision to apply a SARS vaccine would not be taken lightly. Notwithstanding, what type if vaccine might be used?
Vaccines based on mRNA were not mentioned twenty years ago. But as noted above, the spike protein may not be the best immunogen to use:
If SARS coronavirus (SARS-CoV-2) were to re-emerge in humans, its S1 protein might not be the same as that of the 2002-2003 outbreak. Research with IBV has indicated that differences of only 5% of S1 protein amino acids can reduce cross protection. Consequently, S1 differences among SARS coronavirus isolates must not be viewed complacently. The finding that IBV N-protein (major structural protein of the infectious virion) plays a beneficial role in immunity suggests that the SARS virus N-protein should not be overlooked in a SARS vaccine development program.
This paper, published in 2003 and based on a strong foundation of coronavirus pathobiology, neatly summarizes the chronicle of a pandemic foretold. It was not a one-off.
Another perspective can be found in SARS: Future Research and Vaccine (2004) by Yu-Lung Lau of the University of Hong Kong, Queen Mary Hospital. Professor Lau notes at the beginning that “SARS is a new infectious disease of the 21st century that has pandemic potential” and that “the high morbidity and mortality of this potentially pandemic infections demands a rapid research response to develop effective antiviral treatment and vaccine.” SARS was stopped by epidemiologic surveillance and infection-control. Note that treatment comes before vaccines in the original recommendations from NIAID (May 2003):
- Clinical research: What is the presentation of the disease and how might it be managed in the clinic?
- Epidemiology: How is the disease transmitted (e.g., fomites, droplets, aerosols) and what non-pharmaceutical interventions will prevent transmission (masks, air filtration)?
- Diagnostics: How is the disease identified in a patient?
- Therapeutics: What pharmaceutical interventions can be used?
- Vaccines: What is the best approach to coronavirus vaccines?
The reason for antivirals first is that with SARS “an initial viral replicative phase of about 10 days is followed by an immunopathological phase…(and)…the immunopathological response is triggered by the viral antigens, hence the most strategic treatment is to stop viral replication at the initial phase of the disease so that peak viral load and the subsequent damage is minimized.” Thus, future research priorities should focus on antiviral drug screening. There is ample scientific precedent for drug targets, including:
- Virus binding to target cells.
- Fusion of the virus membrane with the cell membrane to allow the infectious particle entry into the cell.
- RNA-dependent RNA polymerase inhibitors to prevent replication of the coronavirus genome.
- Protease inhibitors to inhibit maturation of functional virus particles in the infected cell.
These targets form the basis of anti-HIV therapy that has made AIDS a manageable condition for those who are fortunate enough to receive HAART (Highly Active Anti-Retroviral Therapy, now called ART). [3] There is no reason in principle this will not work for coronaviruses. Moreover, it is still very clear that vaccines against coronaviruses remain problematic, in that durable immunity to coronaviruses through previous exposure or vaccines has not been demonstrated consistently in coronavirus diseases. Given what we (should) know about coronavirus pathobiology, an Operation Warp Speed for SARS-CoV-2 antiviral drugs would have been the stronger partner with the rapid development of COVID-19 mRNA vaccines.
Thus, the overwhelming emphasis on vaccines for COVID-19 has been puzzling from a scientific perspective. Not only should biomedical scientists and those working in BioMedicine (Big Pharma/Big Medicine) know the scientific foundations of coronavirus pathobiology, it is becoming increasingly clear that immune pathology is also associated with SARS-CoV-2 infection. Of course, this was well understood for SARS-CoV when Yu-Lung Lao published his review:
Since immune response might play a role in SARS pathogenesis, one must be cautious of the possibility of enhancement of the disease in immunized subjects. This has indeed occurred for an experimental vaccine directed against feline infectious peritonitis virus, which is a coronavirus. Therefore, caution has been urged on developing SARS vaccines.
Research is beginning to show that T-cell exhaustion and long-term immune system damage follows SARS-CoV-2 infection, especially in people with long Covid. Moreover, the proper testing of candidate SARS and by extension SARS-CoV-2 vaccines would require an animal model that reproduces severe coronavirus disease in humans. During the initial research on a SARS vaccine, macaques were used after being used to confirm Koch’s final postulate that SARS-CoV is the etiologic agent of SARS. [4] However, these monkeys did not always recapitulate the disease state in humans. Early research on the COVID-19 mRNA vaccines used rhesus macaques as the experimental nonhuman primate.
Where do we go from here? None of the foregoing is meant to cast aspersions, but it must be noted that the current COVID-19 vaccines are a rushed and unlikely technical fix for a problem that did not necessarily have to exist. COVID-19 is the third serious coronavirus outbreak since 2002. As has been noted by many, there was every reason to expect another coronavirus outbreak, one that could be worse than SARS or MERS. So far, SARS-CoV-2 is the agent of a worldwide pandemic, and new mutations that make the virus more transmissible and/or virulent have been identified. Given the apparent unpredictability of the course of a coronavirus infection (the sniffles of a common cold, enduring widespread and long-term organ damage, death) there is no good reason that coronaviruses have not remained a continuing commitment in biomedical research since the original SARS outbreak.
But the research establishment clearly did not respond as needed. This is illustrated in the following figure, which is a simple measure (based on entries in PubMed) of SARS, MERS, and COVID-19 research since the original SARS outbreak. As expected, there was a peak in SARS research papers in 2003 and 2004, followed by a decline to a relatively low baseline for such a serious disease>The same was true for MERS beginning in 2013.
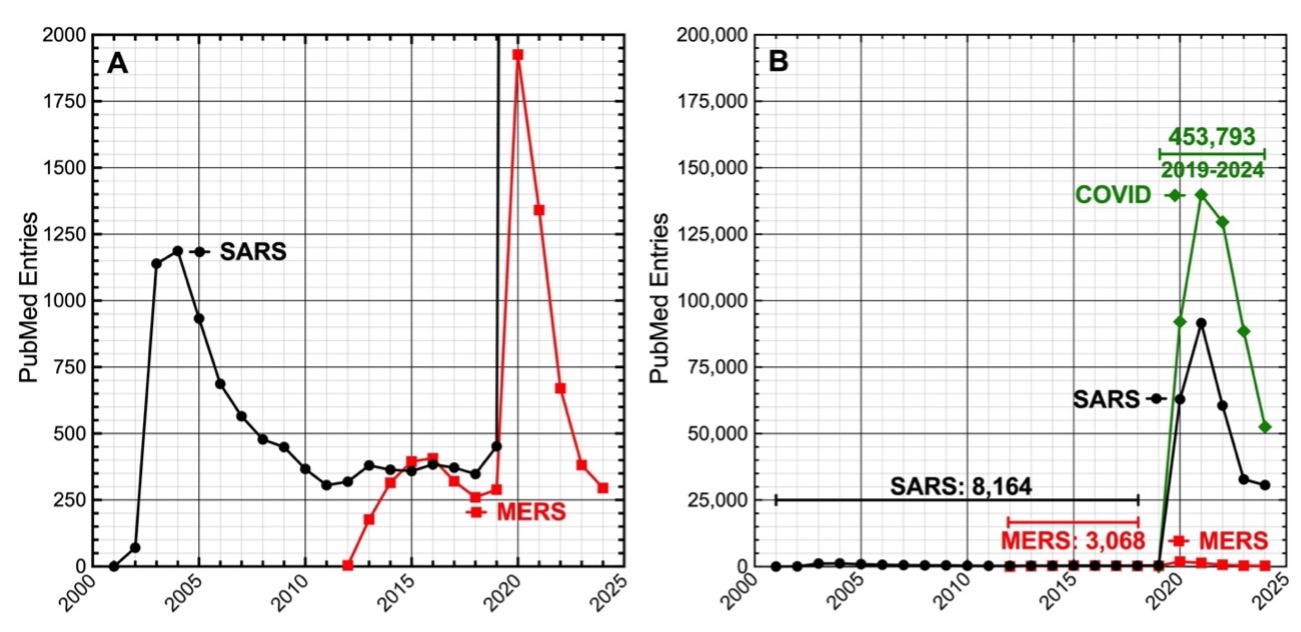
The publication spike beginning in 2019 coincides with COVID-19 (“SARS” as in SARS-CoV-2 would have been included in most research papers on COVID-19). Given the clinical course of SARS and MERS, these two coronavirus diseases should have received more attention. Continued research on viral pathobiology using appropriate model systems, especially on antivirals for human coronaviruses, should have been a high priority of the World Health Organization and the United States National Institutes of Health and similar organizations in other countries with strong biomedical research infrastructures. Alas, this was the road not taken.
The COVID publication spike could represent an attempt by the research establishment to “catch up” as an adjunct of Operation Warp Speed, but it is almost certainly due to changes in the business of scientific publication in the open access era of pro forma peer review in a pay-to-publish environment in which numbers of papers trump content for those evaluating so-called productivity. Note that the scale of the y-axis in Panel A is 1/100th of Panel B. That 454,000 legitimate COVID papers have been published in the past five years is inconceivable. In comparison, as of 23 February 2025, there are 184,856 HIV/AIDS papers in PubMed over the past 43 years.
Where does this leave us? COVID-19 has not disappeared (4,934 deaths in through February 15 in 2025), and the current season has been one of the worst for respiratory infections in a years. Vaccines against SARS-CoV-2 moderate the course of disease in some patients. But they do not prevent the disease or its transmission, contrary what was said by politicians during the height of the pandemic. One year ago a paper appeared in Cell Host and Microbe entitled Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses (the authors are well known and certainly understand infectious disease). A very good article of its kind, the Abstract/Summary is worth quoting in full:
Viruses that replicate in the human respiratory mucosa without infecting systemically, including influenza A, SARS-CoV-2, endemic coronaviruses, RSV, and many other “common cold” viruses, cause significant mortality and morbidity and are important public health concerns. Because these viruses generally do not elicit complete and durable protective immunity by themselves, they have not to date been effectively controlled by licensed or experimental vaccines. In this review, we examine challenges that have impeded development of effective mucosal respiratory vaccines, emphasizing that all of these viruses replicate extremely rapidly in the surface epithelium and are quickly transmitted to other hosts, within a narrow window of time before adaptive immune responses are fully marshaled. We discuss possible approaches to developing next-generation vaccines against these viruses, in consideration of several variables such as vaccine antigen configuration, dose and adjuventation, route and timing of vaccination, vaccine boosting, adjunctive therapies, and options for public health vaccination polices. (emphasis added)
Yes, it has been known for a long time that these agents of the common cold, influenza, SARS, MERS, and COVID-19 are poor targets for vaccines because durable immunity to these pathogens is difficult to establish, either through infection or vaccination. Yet, the goal remains: Develop a vaccine! Perhaps an intranasal killed- or attenuated-virus vaccine will work. Eventually.
The goal is noble, but not at the expense of other approaches that are known to work, including antiviral drugs and non-pharmaceutical inventions. The epistemic closure [5] that led to the overwhelming emphasis of vaccination as the one true solution to COVID-19 was unfortunate but understandable at several levels. The mRNA vaccines were the “hot new thing” in biomedical molecular biology and scientists were enthusiastic about extending this technology to the clinic. That mRNA vaccines had not yet been shown to work against human disease (e.g., Zika virus) was only a technical detail awaiting an inevitable solution. mRNA vaccines were also said to be tunable to new variants in real time, although how vaccinologists could keep up with random variation in SARS-CoV-2 was never explained very well (to my knowledge). And finally, mRNA vaccines were very profitable but possibly not a good business decision, as noted here (paywall) and from a different, more critical perspective, here. It is no accident that Operation Warp Speed was a public-private partnership that favored Big Pharma and Big Medicine.
Finally, that these mRNA vaccines did not work as people have come to expect of vaccines in the prevention of a very serious and seriously disruptive disease has rejuvenated an anti-vaccine movement whose moment has arrived. It will take great effort to avoid this political and scientific Slough of Despond in the coming months and years. More on that in future instalments, but we should also remember that we have also been here before. And that the solution to COVID-19 and other pandemics surely to come will require that biomedical science remember its past while it plans its future.
Notes
[1] To be fair to those pursuing an academic scientific career, well-designed innovative proposals are unlikely to get funded in an environment in which success rates range from 9% to 20%. I am an “n =1” anecdote, but when I attempted to go just beyond current conventional wisdom in a grant application and referred to a fundamental paper published in Science in 1945 by a pioneering cell biologist before cell biology was a discipline, one reviewer was “unimpressed” that a paper so old could be relevant. I note that the first “similar article” at this Novikoff link was The essential role of integrative biomedical sciences in protecting and contributing to the health and well-being of our nation. This is a perfect statement of the role of disinterested biomedical science, especially in the current political climate.
[2] I have visited two CAFOs for industrial pork production. One could not enter the various confinement areas without wearing coveralls and rubber boots and walking through a disinfectant bath. Pigs produce as much or more excreta per individual as humans, so the attached “waste lagoons” are another horrific matter. This is not how livestock should be raised, and those who object to such practices are correct. However, the solution is to go back to a future represented by White Oak Pastures and similar legitimate farms instead of the fever dreams of George Monbiot. The first is sustainable and when extended throughout the Global North it will be affordable as the world gets smaller and economies more local and regional in the coming inconvenient apocalypse. The other, described by Monbiot in Regenesis, is neither sustainable nor affordable. It is most certainly not palatable.
[3] HIV is a retrovirus and inserts its genome into the host cell DNA. Coronaviruses do not do this, but coronavirus infection can persist in the host just as HIV and other viruses (e.g., herpes). The processes of viral entry, genome replication and viral assembly are similar, however, and are good drug targets. Pre-exposure prophylaxis (PrEP) against HIV is also now possible, for those who can afford it.
[4] Koch’s Postulates (strong version): (1) The microorganism must be found in abundance in all organisms suffering from the disease but should not be found in healthy organisms. (2) The microorganism must be isolated from a diseased organism and grown in pure culture. (3) The microorganism (from the pure culture) should cause disease when inoculated into a healthy organism. (4) The microorganism must be re-isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
[5] In prose, as one of my favorite teachers might have put it: If a Scientist A knows vaccines and that a vaccine is the cure for disease X, then Scientist A knows how to cure (or prevent) Disease X. That older wisdom is inconsistent with this matters not. Epistemic closure has led biomedical science down other “unproductive” pathways, including the Diet-Heart Hypothesis that led to the demonization of a balanced, omnivore diet and caused an obesity epidemic; and the Amyloid Cascade Hypothesis of Alzheimer’s disease, which has yet to suggest an effective intervention for AD. My first and indispensable mentor in science, an enzymologist of the old school, never transcended his epistemic certitude that only enzymes (proteins) could have catalytic activity and nothing could convince him otherwise, even after Thomas R. Cech and Sidney Altman were awarded a Nobel Prize in Chemistry for their discovery of catalytic RNA. Still, we could do with a few more of those sages from another world.


> However, these monkeys did not always recapitulate the disease state in humans.
> but should not be found in healthy organisms.
Asymptomatic transmission was confirmed no later than May 2020. How confusing was this for using Koch’s Postulates as guidance?
Compare to traffic deaths:
: The model forecasts total traffic fatalities for January 2025 to be 3,380.
> COVID-19 has not disappeared (4,934 deaths in through February 15 in 2025)
The two are tracking almost identically, but we don’t have legislation brewing against seat belts.
But people don’t “die suddenly” while wearing seatbelts. Also one would have to compare accident death rate before seatbelts to accident death rate with seatbelts. It is difficult to get the current death rate with the current “seatbelt” use compared to those that chose not to wear said “seatbelts”. I know I have been trying.
IBV indeed.
Everything about how the vaccination fiasco was going to unfold was known long before the pandemic even started.
And yet…
Also, quite disturbingly, it is not just malicious intent to bamboozle the public. There certainly was a lot of that on the political side, and the coronavirus experts who never spoke out are guilty as charged of going along with that plan.
But if you quiz very prominent virologists on what they know about IBV **today**, forget about five years ago, you quickly realize they have no clue. As incredible as that might sound and as inexcusable as it is.
The reasons are many:
1) Big shot PIs are not in the business of learning things, they are in the business of being managers of an operation. Grant money comes in, publications go out. Learning doesn’t really feature in the process as an objective beyond what is minimally necessary to sustain it (and often even that does not happen). They have neither the time nor really the inclination.
2) The absurd implicit anthropocentric notion that humans and everything else alive are separate things, and therefore that what diseases other animals get is irrelevant, is still very widespread. Thus IBV in chickens is just something nobody has any interest in learning anything about, and that is an active bias beyond the general apathy towards learning.
3) It is also not sexy. Veterinarian medicine research? Who cares, that won’t get you into prominent single-letter journals. That sort of work gets published in obscure journals that only the people who publish in them read (and often not even they).
And so on.
When your top “experts” are overcredentialed, undereducated, and motivated by incentives all going in the wrong directions, this is what you get…
I am no virologist but a backyard chicken owner. What is completely missing in this piece is the most pertinent fact: I.e. that keeping millions of chicken in completely unnatural and unhealthy conditions will of course result in disease. Medical interventions will not change the underlying conditions but will just result in more dangerous pathogens. That is the history of Mareks disease. Marek was in the beginning a disease that will kill from 5% to 10% of chicken held in mass cages. Now it is absolutely deadly for any non vaccinated chicken. I wouldn´t be surprised if medical intervention in factory farming will lead to pathogens that are deadly to humans as well. Not that anybody will research that. Our science departments rely on “third party money” and everybody knows where that comes from.
About the Covid vaccine: absent from the above piece is the fact that the Pfizer and Moderna shots have resulted in more adverse effects reported to VAERS (vaccine adverse event reporting system) than all other vaccines for the last ten years combined. One can endlessly argue about the significance of this but surely it at least rates a mention. Curiously here in Germany our equivalent to the CDC has not been able for four years to parse the health insurance data for adverse events related to the above shots. And that although it was mandated to do so by the Bundestag. So altogether the above is an interesting piece but unfortunately only a look at part of the problem.
It’s a bit buried but have a look at footnote [2]. There, KLG points to pork farming practices and notes: “This is not how livestock should be raised, and those who object to such practices are correct.” As an example of a better approach, he links to White Oak, which also handles poultry. Your point is compelling, though: current industrial agriculture is unsustainable, to say the least.
Thanks, you’re right. Still I wonder why the author hasn´t been able to think outside the box. It’s a bit disturbing as he seems highly competent. Why look for the solution to a problem that shouldn´t exist in the first place? Also what about immunity? My neighbour is an organic farmer and he firmly believes most outbreaks of animal diseases are due to the degraded immunity of factory farmed animals.
The entire episode is a form of epistemic closure on steroids. I find it unreal how many times I raise the subject and just get blanked out – people (especially the PMC adjacent) simply don’t want to discuss it.
I think the primary explanation is the knowledge that acknowledging the numerous public health and scientific failures will inevitably do even more damage to the status of PMC elites. The damage caused to the principles of good science and public health is immeasurable.
The “PMC” is comprised of the P’s and M’s who are able to prosper (or at least survive) in a system where they are beholden to the political establishment and the wealthy. The P’s and M’s who can’t or won’t are silenced or excluded.
It has long been odd to me how the PMC are so reluctant to admit mistakes and generally seem to double done on their errors. I have always found that an acknowledgment and an a sincere apology go a long way to keeping respect and good relations intact.
Otherwise, belated thanks to KLG for this retrospective. A good reminder that I am not the crazy one. This whole COVID public health debacle has done so much to weaken my faith(?) in the good of humanity. In spite of how low what has really been going on has brought me, I will always be grateful to Lambert and the COVID brain trust for staying on top of this for all these years.
The only real way that this Pandemic should have been handled is by an empirical approach. IM DOC said early in the Pandemic that you can’t vaccinate your way out of a Coronavirus and this was taught in medical schools. That fact alone should have shown us what was and was not possible. Instead the Pandemic was handled with the idea of political expediency in mind which came up with “magic bullets” aka the vaccines. And when time proved how false those hopes were, Biden declared the Pandemic over so get back to work. And that was it really. The desire to save the economy of 2019 and not to have to change anything. Too many people were making money with the old economy and business leaders fought tooth and nail to try to keep everything the same, no matter how many people died. They were considered “acceptable loses” though Long Covid was an unplanned for spanner in their plans. And if the next Pandemic is also spread by aerosols, they will do the whole thing all over again and you can bank on that.
All true, though it strikes me that is one thing for an ordinary layperson to go along with the “magic bullet” discourse and another for those who are considered experts in medicine and virology.
Numerous other MDs had the same textbooks that IM Doc had. Did they all just forget that there has never been a vaccine that was effective against a coronavirus? Why did so many go along with the hype about the mRNA technology? IM Doc was skeptical, but evidently many of his peers were not. And KLG’s article makes it clear that even decades later, in the early 2000s, there was solid research done on SARS and MERS.
So what happened?
The answer to this question is above my pay grade, but one of the points I take from this article is that with the SARS-CoV-2 epidemic, biomedical science failed to “remember its past” in a rather spectacular fashion, and give the magnitude of this failure — still ongoing, to boot —, it’s difficult to believe it won’t happen again on an even larger scale.
Of course we docs were skeptical. But in the midst of of a novel and deadly airborne viral pandemic, we were all scrambling for answers and solutions. Thus the necessary rapid push for vaccines by Trump. Early vaccine trials were favorable, and they quickly took over from HCQ.
“The necessary rapid push for vaccines by Trump”
That to me is the entire point of the debacle that this has all become. I heard from many coronavirus expert virologists very early on in this entire situation. I heard them speaking in public before they were censored completely by the profession. Without exception, they were stating that vaccines were never going to be the answer. Vaccines in all kinds of forms had failed repeatedly in coronaviruses in human and animal experience. That the only way out that was safe in the long run was to protect the most vulnerable, to protect ourselves, and to let the war run between our collective immune systems and the virus. They were allowed to speak for a few months – but then once the lucre started to flow the profession and the pharma/media complex had them shut down upon pain of losing everything.
I disagree with you wholeheartedly. A few docs were skeptical. They asked questions. But if they dared say anything against the ever-changing narrative, they were ridiculed, delicensed and deboarded. Instead of rationally and via the scientific method being allowed to find answers – the top-down tyrannical censorious approach was used. The entire population saw this – and the media and likely the medical profession will never be the same for it. Early vaccine trials were never favorable. As someone who sat on IRBs for years – every trick in the book was applied to them. There is no way to make that claim with a straight face when the control groups were immediately terminated in all of them. That is what I would call an “original sin”. It completely destroys any ability to assess safety issues, and it completely destroys any ability to follow up on long term efficacy. But our profession acts like today this was all OK. It was not and is not. At the same time, I have about a dozen or so veterinarians as patients. Old and young. And to the one – they refused vaccination. They saw what this had done in animals over time and had no desire for it to be done to them and their families. All are still alive and well. WHAT DID THEY KNOW THAT ALL OF OUR DOCS DID NOT KNOW? AND WHY WAS NO ONE LISTENING? We as an entire society are going to pay for this dearly – it has fueled an anti-vaccine movement that has shocked even me. I find myself daily dealing with patients over and over again that are deeply skeptical of any vaccines.
The profession of medicine is going to have to go through the “valley of the shadow of death” for the next generation or so. We are going to have to do all we can to re-earn the trust that was lost. All the mealy-mouthed crap coming out of our leadership and pharma right now is just not going to cut it. We have not bothered to police our own – so now it will be done for us.
Thankfully, I am seeing many signs in the students I teach of the massive backlash that is brewing. I would argue that the current students are the vanguard of what we call Gen Z. They bristle at the idea of top-down dictates, they ask very hard and tough questions, and they seem to be really disturbed at what has happened, the lying and dissembling, over the past 4 years, they are extremely skeptical of the current corporate medical model controlled by Pharma, Insurance and hospital corps. I am actually quite surprised by this.
This is why I still work. I can retire at any time. But first of all who would take care of my patients that I so care about, a bunch of NPs who were trained via correspondence school, or med school grads from the last 20 years who really know a lot about things like equity but have little understanding of medicine? But more importantly, these very young kids who are in my opinion showing much promise are going to need some old gray-hairs around.
The first part of my career was defined by AIDS and the many disasters brought upon the population by our agencies and public health. The middle part of my career, still ongoing, was defined by the opioid epidemic and the disasters brought upon the population by our agencies, public health and Pharma. The end of my career will be defined by COVID and the many disasters brought on by our agencies and the horrific public health response and the obvious overarching corruption for all to see. I just cannot stop right now.
And thank you KLG – we will be discussing this at our next journal club.
“That the only way out that was safe in the long run was to protect the most vulnerable, to protect ourselves, and to let the war run between our collective immune systems and the virus.”
There is no way to “protect the most vulnerable”. The most vulnerable don’t live in a bubble. Many elderly people live with their grandkids who go to school. They live with their kids who don’t have the luxury of working from home. Immunocompromised kids have to go to school, unless their parents home school them.
Immunocompromised teachers can’t just teach remote.
Like antidic, I strongly object to this remark:
“That the only way out that was safe in the long run was to protect the most vulnerable, to protect ourselves, and to let the war run between our collective immune systems and the virus.”
Who said this besides the Great Barrington Declaration authors? The rest of the scientific community was horrified by their declaration, as you may recall.
Of course few docs early on felt that we could produce a significant and tested vaccine in a relatively short time, but what other choice was there?
Then when the mRNA technology was explained, many of us felt we should give it a try. The coronaviruses being notorious for mutation might be reined on a longer term basis since the mRNA technology might be able to keep up. I still don’t know what else we could have done. Trying to isolate the elderly and other high risks, possibly a 1/3 of our people, was no easy task. Especially in the longer term.
*Sigh*
Vaccines were not the only protection. A school district in IM Doc’s area has been strict about masking and ventilation and making kids go home when sick and not return until recovered, and I believe they use the old standards as for how long to isolate after a positive Covid test (IIRC ten days). They have had a tiny fraction of the Covid cases in other schools.
Similarly, I am in Southeast Asia. There was widespread masking well into 2023 (due to masking being seen as polite, to frequency of high PM2.5 pollution days leading to regular masking, and memory of SARS). Covid rates across the region were MUCH lower than in the US.
And ….. if a doc’s “scrambling for answers” veered away from the corrupt CDC/NIH propaganda, that doc was fired or lost their license. Not too complicated as to why the response has been a failure.
Can´t really blame docs. They have a lot to do and must rely on FDA, CDC et al. Problem is the total corruption of science thru “third party money” and the revolving door agencies.
The trials were conducted by Pfizer and Moderna on their own products. A clear conflict of interests. It’s since come out that some of the trial data was massaged, or misreported, as they say. / ;)
Looking forward to new standards for legitimacy in trials, informed consent, objectivity, replicability, independence, explicit disclosure of conflicts of interest, related parties and comprehensibility for any and all lay readers.
Repetitive, I know, but written in the spirit of eliminating legalese loopholes and ambiguity.
Wish list addendum: eliminate blanket liability and enforce pharma exec and board accountability.
And an FDA official just joined Pfizer.
Keep that revolving door going 3600 RPM
While there definitely had to have been some health professionals who were complicate or happily ignorant, I think you also have to take into account the fact that there were varying degrees of threats against anyone in the medical world who openly recommended any other approach to the disease. And it appears there was also in some places if not everywhere a solid gaslighting campaign against medical professionals. Just last week I was watching a video where an prominent and retired Australian oncologist said that early into the pandemic he raised concerns to the Australian health department leaders about the approach the were rolling out. He was told his opinion was only of a tiny minority. He goes on to explain that more recently while at a conference (or some other gathering of medical professionals) that the topic of how the pandemic was managed was discussed and lo-and-behold several in the group had done the same thing and all had been told a similar line that they were the only one with a concern.
At the beginning of the pandemic, in 2020, RT had a 30 min interview with the Scientific Director from the Gamaleya Institute of Virology in Russia. He also poured a lot of cold water on the idea of a long term, full immunity vaccine for COVID.
“And if the next Pandemic is also spread by aerosols, they will do the whole thing all over again and they can make bank on that.”
Fixed it for you, Rev.
Call me cycnical but if you insert words like ‘profit’ and ‘greed’ and ‘opportunity to further own interests’ etcetera you get a better idea of why certain things were ignored and why other things were done the way they were. Politicians had power and wanted to capitalise on the opportunity while those wanting to make bank had the reigns over science. Anyone who disagreed with ‘The Science’ as approved by those in control was labelled a pariah.
I apologize if this is perhaps only adjacent, but it seems to me that powerful, moneyed forces were determined that anything would be preferable to the expense necessary for an investment in improved indoor air quality analogous to the public works of 19th century London to control the scourge of waterborne illnesses. And I mean literally anything — death and debilitation be damned.
The oft repeated claim that vaccinated folks were protected from severe COVID-19 and hospitalization is not mentioned in these discussions. Is this claim untrue?
I believe it to be true, and very important with the earlier Covid variants. I followed data locally, state based (AZ), ID, OR, CO and WA. And for a large part of 2021/2, they all said the same thing. That being your chances of ICU admission or death were much higher if you were not vaccinated. As the virus mutated to a more benign state with the Omicrons, this effect gradually became less pronounced.
Yeah. I was recruited to the REACT study as the pandemic started. Thanks to our crappified/privatised postal service my at home kit in early 2020 had clearly been tampered with when I received it. I couldn’t get a valid result when it was clear I’d had COVID (badly – I was very close to calling ambulance during the night but I have absolutely no time for my local hospital A&E).
Thus I never got followed up. I’ve had COVID probably 4 times but only once is clinically documented (when I stepped up to help in admin in oncology in local hospital and caught it there and had to be properly tested and work from home). Ironically they didn’t like another positive test and stopped calling me back to do shifts there. Sheesh.
I found this very interesting study on Covid infection in the Los Angeles area sorted by income deciles on the CDC website. Apparently people in the lowest income decile were five times more likely to get Covid than the top income decile during the first wave, four times more likely in the second wave, and about fifty percent less likely in the third wave. The vaccines were introduced just after the second wave.
My memory from reading other studies is that deaths spiked in the first and second waves, but did not during the third wave after the vaccines were introduced. Of course, everyone said: ‘The vaccines saved us.’ They also said that post-omicron Covid was milder, though I don’t think this has been definitively proved.
I think there are other possible explanations:
1). Those who were most vulnerable, and were likely to die, had already died.
2). The people who got Covid in the first two waves probably had more comorbidities than those who didn’t, as wealthier people were more likely to be healthier as well as to be able to work from home and isolate themselves.
3). These wealthier deciles ended up getting more Covid in the third wave because they were likely fully vaccinated and thought themselves invulnerable. But, since they were healthier anyway, this didn’t result in a spike in deaths.
I’m hope someone will eventually be able to sort the data and determine how much of the improvement in the Covid death rate in the third wave was the result of vaccines, how much was the result of the changing lethality of the virus itself, and how much was the result of healthier people getting Covid.
https://www.cdc.gov/mmwr/volumes/72/wr/mm7226a5.htm
I was struck while reading this very good piece that there was a massive difference between the “early” coronavirus outbreaks (SARS and MERS) and the COVID outbreak.
The first two, although serious for the people affected, seem to have been limited in geographical scope, were shut down rather quickly, and after a few years disappeared as a matter of widespread medical concern. COVID, otoh, as we have seen, quickly spread to most of the global population and does not show any signs of going away in the time since it was first discovered.
An interesting question to my mind is why this major difference occurred. One possibility is biological differences between SARS and MERS viruses on the one hand and the COVID virus on the other. I’m certainly not qualified to speak on that although there seems to be an overall similarity between the two groups.
Another possibility is changes in human society that make humans in 2020 vastly different from humans in the early 2000s when it comes to their propensity for spreading a coronavirus. I have always thought and still think that COVID was largely spread by international and intercontinental air travel. Even symptomatic carriers can travel anywhere in the world in the 2-3 days it takes for symptoms to appear. And of course half of COVID carriers never show symptoms at all.
And yet, have there been massive changes in air travel in the last two decades that would allow this to be an explanation of why COVID spread much more widely?
I’d appreciate hearing from anyone who has any insight on this.
Lambert Dec 11 2020: We’ve seen a million fingerwagging posts about bikers and Sturgis, and virtually nothing about international air travel that infected the whole country to begin with. Odd.
[I did see a more recent article that supported large increases in air travel, but can’t find it. So many articles…]
I would add something that is still not fully worked out.
There is very compelling evidence to believe that Coronavirus OC43, in universal circulation among humanity right now and the cause of cold-like symptoms and not usually fatal, was the etiologic agent of what is now known as The Great Russian Flu of the 1890s.
It is important to note that medical commentary at the time was struggling with this pandemic, it was called a “flu” but they were all pointing out that the symptoms were not exactly the same as a flu. It had much in common with COVID from our era. It will be very difficult to ever prove this to be the case, but the evidence is very compelling. The other fascinating thing that happened during that episode was when it first got started it was highly pathogenic and many died. This was written about in the literature of the time – most notably the Sherlock Holmes canon. By the end of the decade of the 1890s it had significantly calmed down and very few were getting too ill, much less dying.
This could be a analog to COVID 19 in our own time.
Thank you KLG for a very informative writeup, you are an excellent technical writer and have produced some of my favorite articles here at NC.
I would like to point out another thing that was well known long before COVID — differential equations as the basic modeling tool of epidemiology. Early in the pandemic I was sceptical that we had quickly invented a vaccine for SARS-COV2 because I had always read that coronaviruses mutate very rapidly, and that is why we have never had vaccines for influenze and the common cold. So I dug in the attic and found my old Diffy Q homework where, sure enough, we had problems about the spread and control of disease, along with population growth, bacteria growth, diffusion and mixing in fluids, etc. In my non-Ivy, Diffy Q was a senior level class in the College of Mathematics, and a requirement for junior level work in Engineering (my profession). So after a bit of brushing up, I started looking at the pandemic and its (lack of) responses largely from that standpoint.
Diffy Q is a surprisingly broad field, but I would take a simple statement from God Emperor Fauci himself to illustrate the basics. We want to know if a bunch of things that are changing with respect to a common variable, time in this case, converge on the desired solution. Very early on in the push for the vaccines Dr. Fauci made the statement that “If we can just vaccinate 50% of the population, this will all be over in 2 weeks.” (It is easy to find supercuts of him stating every percentage above 50% as well as the marketing progressed.) A critical analysis of that statement would start with a simple truth test — clearly it is false as we reached vaccination levels far above 50% and it most assuredly did not end in 2 weeks. Those numbers presumably represent a percentage of the population who are now immunized, and a time period for the disease to rip through the other half of the population. In short, he is trying to state that a0, or r0, or whatever your term of choice, has to be below 1, each infected person must infect less than one other person. Good so far, but America’s Top Doctor and Leading Infections Disease Expert would get an F at my lowly flowover university — the correct answer being more like “If we can vaccinate 50% + 1 (!) of the population with a vaccine that is 100% effective at producing immunity for the lifetime of the recipient, it will all be over in t time periods, where the total time depends on such things as the infectivity rate of the virus, the susceptibility rate of various segmets of population, the mutation rate of the virus, the mixing rate of the infected and uninfected populations, the length of contagion among the infected, and probably quite a few more factors, all of which vary over time.” Proper NPIs can affect those rates, as can quarantines, and ventilation, and non-approved treatments, and testing and monitoring to know when to update the mix of things you need to do for control. The WHO’s definition of vaccine prior to September 2021 takes a shortcut compared to my runon sentence — a substance that produces immunity in at least 50% of those vaccinated for a period of at least one year. Note that their time period is far more useful than Fauci’s, you need enough people immune long enough that you can manufacture, distribute, and apply more of it before the first recipients get sick again, and that necessarily implies that the underlying pathogen has not changed significantly as to render their immunity null.
I began following the Variants of Concern report from UK Health Services based on a link here at NC, and the April 2021 release showed that immunity against infection was in the mid-30% range among several age groups after 12 weeks (delta serotype now prevalent?). In my mind this is the day it went from “potential vaccine” to “failed vaccine”, yet we would be subject to several more months of “pandemic of the unvaccinated” and “rare breakthrough” marketing campaigns, ending in the August 2021 declarations by President Biden and CDC Director Walensky that fully vaccinated people could neither contract nor spread the the disease — months after we knew it was not a vaccine useful for preventing the spread of COVID. Then quietly in mid-September 2021 the WHO and CDC changed their defitions of vaccine to remove any mention of immunity. In essence they simply changed the definition to match the product they had — a substance that stimulates the immune system to provide an increased probability of a less severe outcome. “Increased probability” and “less severe” are terms for the marketing and legal department, not scientists and not public health campaigns. Can anyone remember when every kid in your elementary class got the polio vaccine every year, contracted polio almost every year, but was less severely crippled as a result?
Another stab at Saint Fauci is in order here. During his hagiography interview with the NYT (late 2023) he made the statement (paraphrasing) — “We were used to vaccines whose durability was measured in decades, and these vaccines had durability of a few weeks, we just didn’t know!” B*llsh*t Tony, you knew. You knew it no later than April 2021, you knew that meant it was not an immunizing vaccine, and yet you continued on with a vax-only policy. That lie has lead directly to the credibility issues mentioned in KLG’s article, along with an uncounted number of deaths. My generation is staunchly pro-vaccine, we didn’t get polio or mumps or measles or several others, and you managed to destroy that good will. No vaccine provides perfect immunity or is perfectly safe, they cost money, they take time out of your life, they can make you sick, etc. but we all did that because public health policy mattered. And people wonder where “vaccine hesitancy” is coming from FFS? The most important currency in public health is credibility, and it is shot.
And that brings me to another simple thought experiment that illustrates differential equations as applied to infectious disease — initial conditions and time offsets. A worker takes a blood sample from an infected patient, that blood sample is DNA sequenced and studied, a proposed mRNA vaccine is designed, a production process has to be designed, then it must be produced, distributed, applied, and given time to take affect. (NOTE: I have left out the testing phase as that is apparently no longer important.) Now take an indiviidual who just contracted COVID (and survived) and compare them to the freshly vaccinated individual — whose antibodies are more current/correct? A doctor friend assured me that this was nonsense, the reports he was given showed the neutralizing antibody titers were off the charts in the vaccinated. My reply — what level of now-out-of-date antibodies is better than the current ones the patient just generated? Mandating vaccines for the recently infected caused them to burn some of their finite number of naive T-cells just for a software downgrade. I should also point out that the idea of herd immunity to COVID suffers from the same issues as mRNA vaccines when it comes to trying to defeat the mutation rate monkey.
Finally I would say a few words about the word “vaccine”. I have >30 immunology and epidemiology texts (RIP Aaron Schwartz) which are now a few years out of date, and I spent considerable hours studying terminology and the math used. I will say that among immunologists and researchers, vaccine is indeed just a drug that affects the immune system. But in public health it has historically meant IMMUNIZING, and that sleight of hand is the problem in a nutshell. Playing on the stupidest timeline and wordplay common here on NC, I propose the following additions to our language to help people differentiate between the types of vaccines that the overworked word vaccine must now cover:
TradVAX These vaccines create IMMUNITY to the pathogen of interest in a sufficient percentage of recipients and for a period of time long enough that they can be used to control, and in some cases eliminate disease. They must be applied prior to contracting the disease. Think polio, think MMR. These drugs benefit the public at large.
FauxiVAX These vaccines confer an increased probability of a less severe outcome of a disease, where “increased probability” and “less severe” are left up to the interpretation of whoever is in charge at the moment. They may have undergone some safety testing, and must be applied prior to contracting the disease. Think mRNA COVID vaccines. Also, now you can put Flu Vaccines (formerly Flu Shots) in this category. These drugs can benefit an individual. Their only use for the public at large is to possibly smear out in time a surge of illness that is overwhelming PE-reduced hospital bed counts — the area under the curve is unchanged in the long run.
Thera(nos)VAX These vaccines can cure non-infectious disease like pancreatic cancer*, and are taken after you contract the disease. In the past we would have called these therapeutics, or perhaps gene-therapy products (just as we should have called FauxiVAX if we were being honest). One side effect of these vaccines is that they eliminate that viral (sorry) misinformation marketing ploy, one of which was so righteously destroyed by our host regarding an internist in GA, where suddenly everyone begs for vacccines in the ER and has to sadly be informed that it is too late.
It is difficult to look at our public health leadership during COVID and not think of this: https://www.youtube.com/watch?v=uTmfwklFM-M
*I refer to an article here at NC by KLG which describes a very promising new treatment for a certain type of pancreatic cancer. Incredibly good news, great use of technology, but …. vaccine??? Well… it is now!